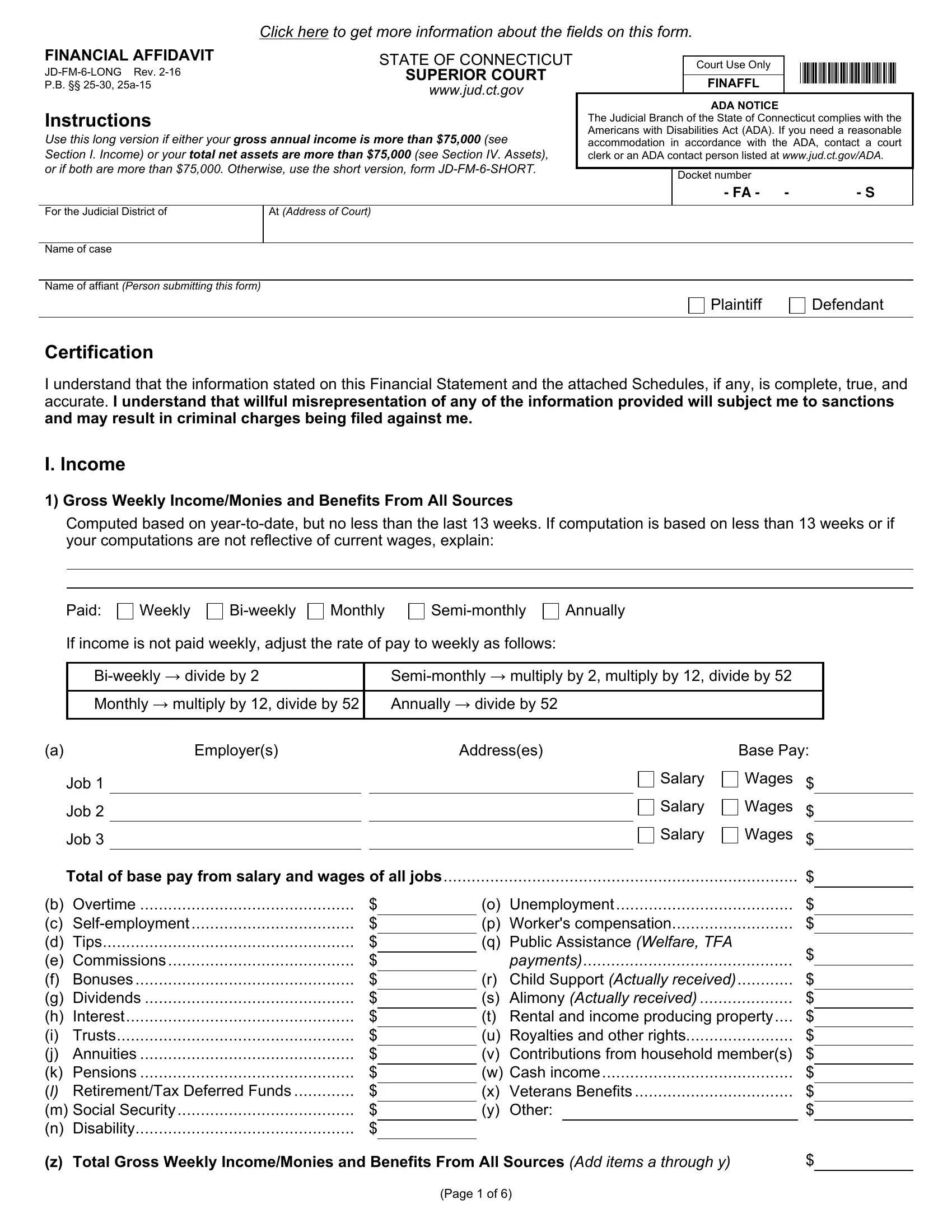
In the intricate landscape of legal documentation, the JD-FM-6 Long form stands out, particularly within the judicial framework of Connecticut. As a financial affidavit required by the Superior Court, its primary function is to meticulously document an individual's financial status, providing a comprehensive snapshot of income, assets, liabilities, and expenses. This form, reserved for cases where either gross annual income or total net assets exceed $75,000, demands meticulous attention to detail. It guides the filer through various sections, each designed to capture different facets of financial health, from weekly income and mandatory deductions to the subtleties of weekly expenses not deducted from pay. Further sections delve into the realms of assets and liabilities, delineating categories that include everything from real estate and motor vehicles to retirement plans and insurance. The form also makes provisions for disclosing the assets of any children involved, ensuring a thorough accounting of family finances. Designed with rigor, the JD-FM-6 Long version ensures that the court receives a clear, accurate, and complete picture of an individual’s financial standing, which is crucial for making informed decisions in cases where financial matters are at issue. The seriousness with which this form must be approached is underscored by a certification that all information provided is true and accurate, highlighting the grave legal implications of willful misrepresentation.
| Question | Answer |
|---|---|
| Form Name | Jd Fm 6 Long Form |
| Form Length | 6 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 30 sec |
| Other names | what ct form financial affidavit, ct financial affidavit jd fm 6 long, financial affidavit state of ct, jd fm 6 financial affidavit |