
Jv 220 A Form can be filled out easily. Just open FormsPal PDF editing tool to complete the task promptly. To have our tool on the forefront of practicality, we aim to integrate user-driven capabilities and enhancements on a regular basis. We're always looking for feedback - play a pivotal role in remolding how we work with PDF docs. Here is what you'll want to do to get started:
Step 1: Just click the "Get Form Button" above on this page to start up our pdf file editing tool. Here you'll find all that is needed to fill out your file.
Step 2: With this online PDF file editor, it's possible to accomplish more than simply fill in forms. Try all the functions and make your documents appear high-quality with custom text put in, or optimize the file's original content to excellence - all that comes along with an ability to add any images and sign the PDF off.
Completing this document calls for thoroughness. Ensure that all required blank fields are done accurately.
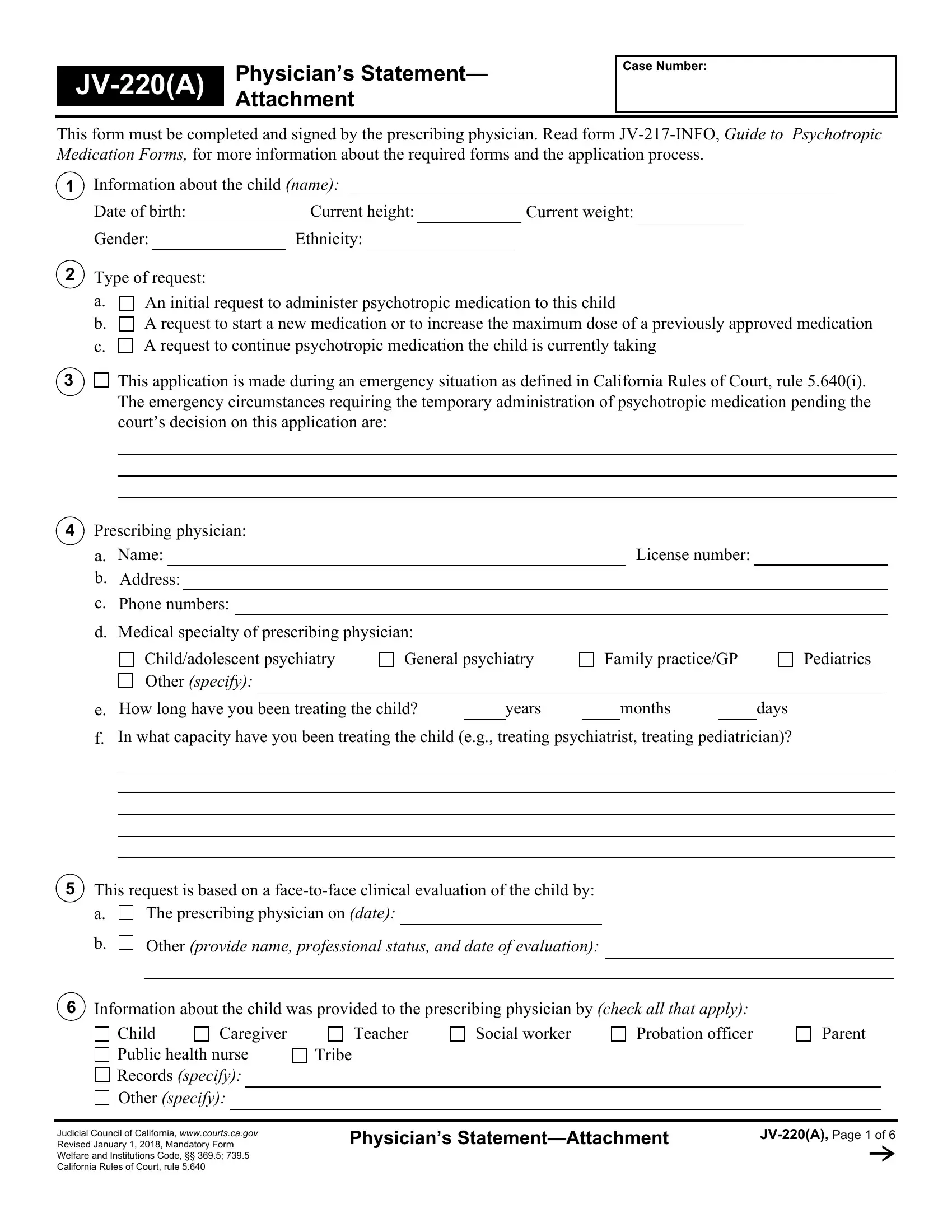
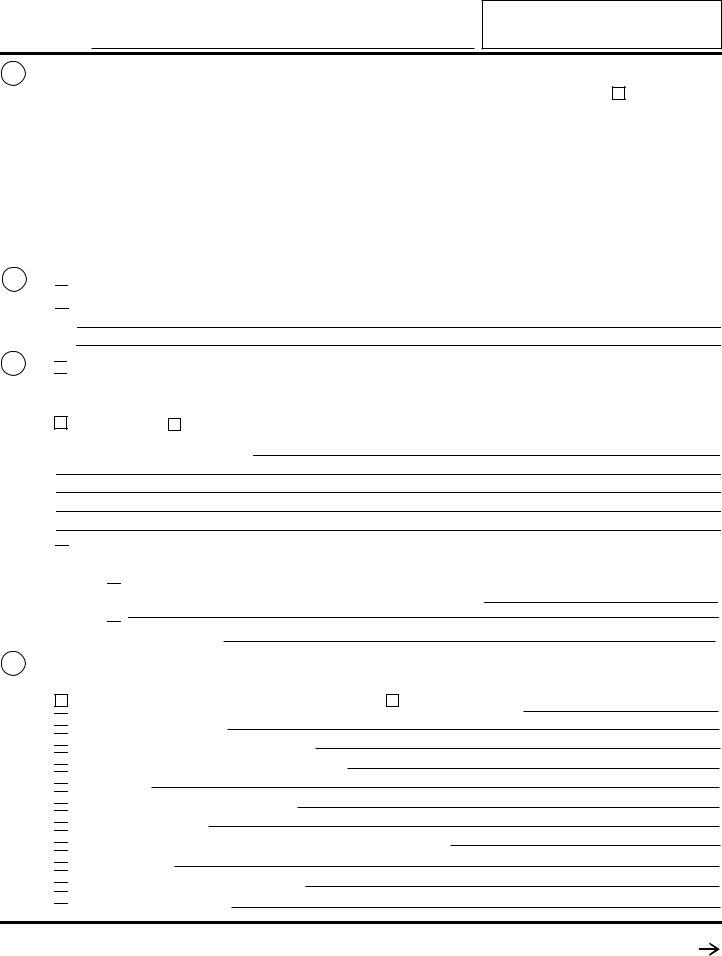
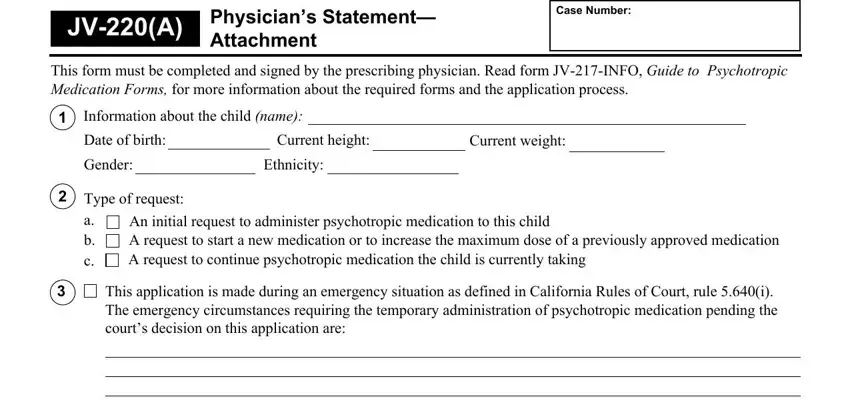
1. Begin filling out your Jv 220 A Form with a group of major blank fields. Gather all the important information and make certain nothing is left out!
2. Soon after filling out the last part, go on to the subsequent stage and fill in the necessary particulars in these fields - Prescribing physician, a b, Name, Address, Phone numbers, License number, Medical specialty of prescribing, Childadolescent psychiatry Other, General psychiatry, Family practiceGP, Pediatrics, How long have you been treating, years, months, and days.
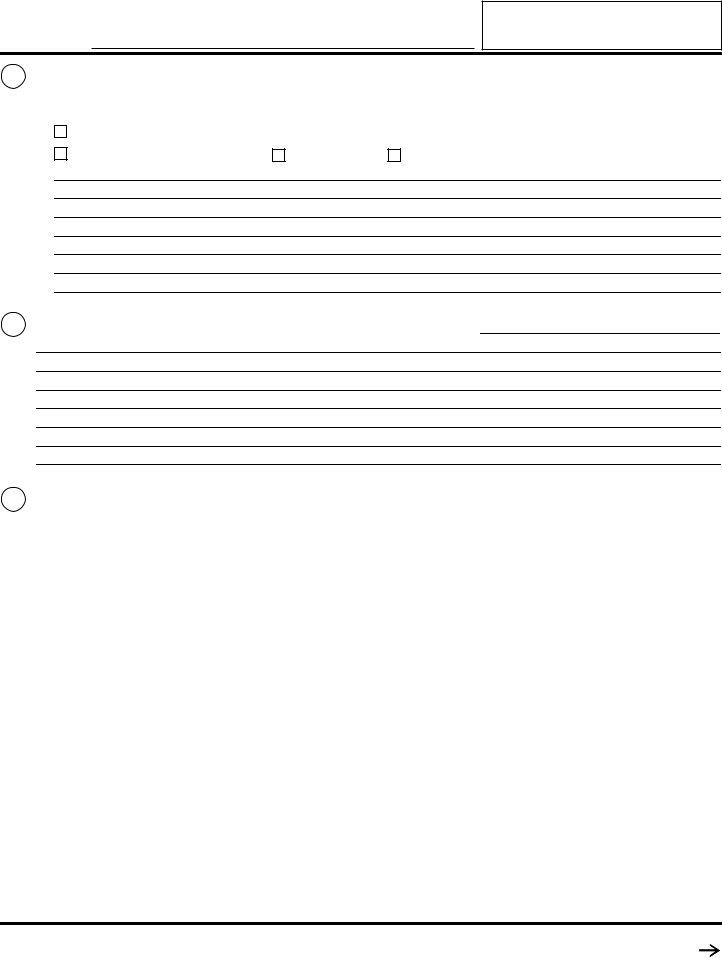
3. This next segment should be pretty uncomplicated, Caregiver, Child Public health nurse Records, Tribe, Teacher, Social worker, Probation officer, Parent, Judicial Council of California, Physicians StatementAttachment, and JVA Page of - all of these empty fields must be filled in here.
4. To move ahead, your next part will require completing a handful of empty form fields. Examples of these are Provide to the court your, I dont know, Describe the childs symptoms, and I dont know, which are integral to continuing with this form.
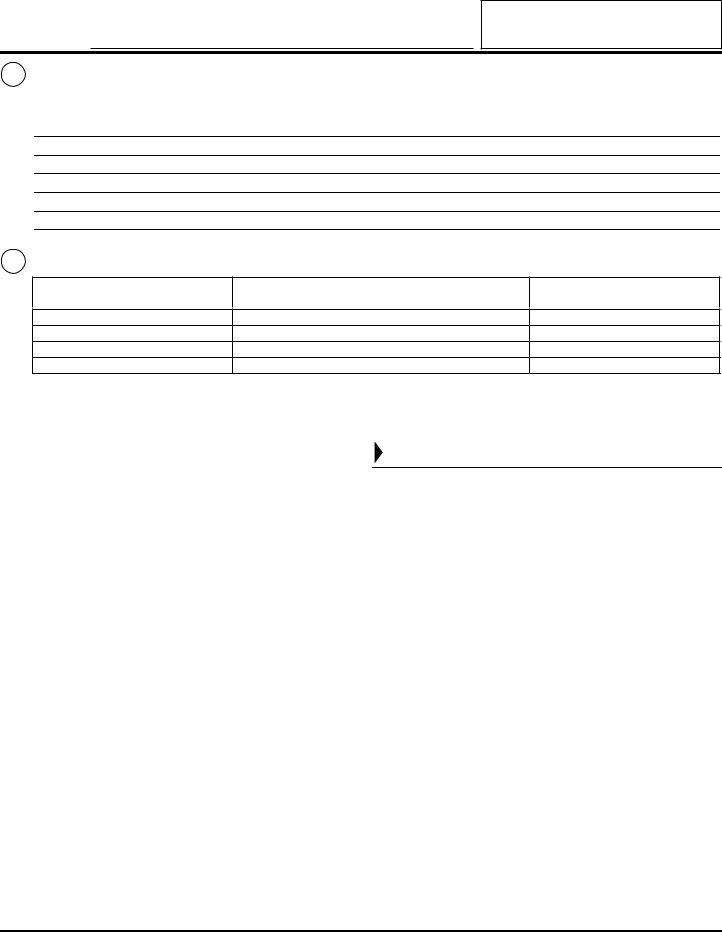
5. The form has to be finalized by filling out this segment. Further one can find a comprehensive list of blank fields that have to be filled in with correct information for your form submission to be complete: Describe the childs response to, I dont know, Describe the symptoms not, and I dont know.
People generally make some mistakes when filling out I dont know in this area. Ensure that you review everything you type in right here.
Step 3: After rereading the filled in blanks, click "Done" and you're done and dusted! Go for a free trial account at FormsPal and obtain direct access to Jv 220 A Form - download or edit inside your FormsPal account. Here at FormsPal, we do our utmost to ensure that all of your information is stored secure.