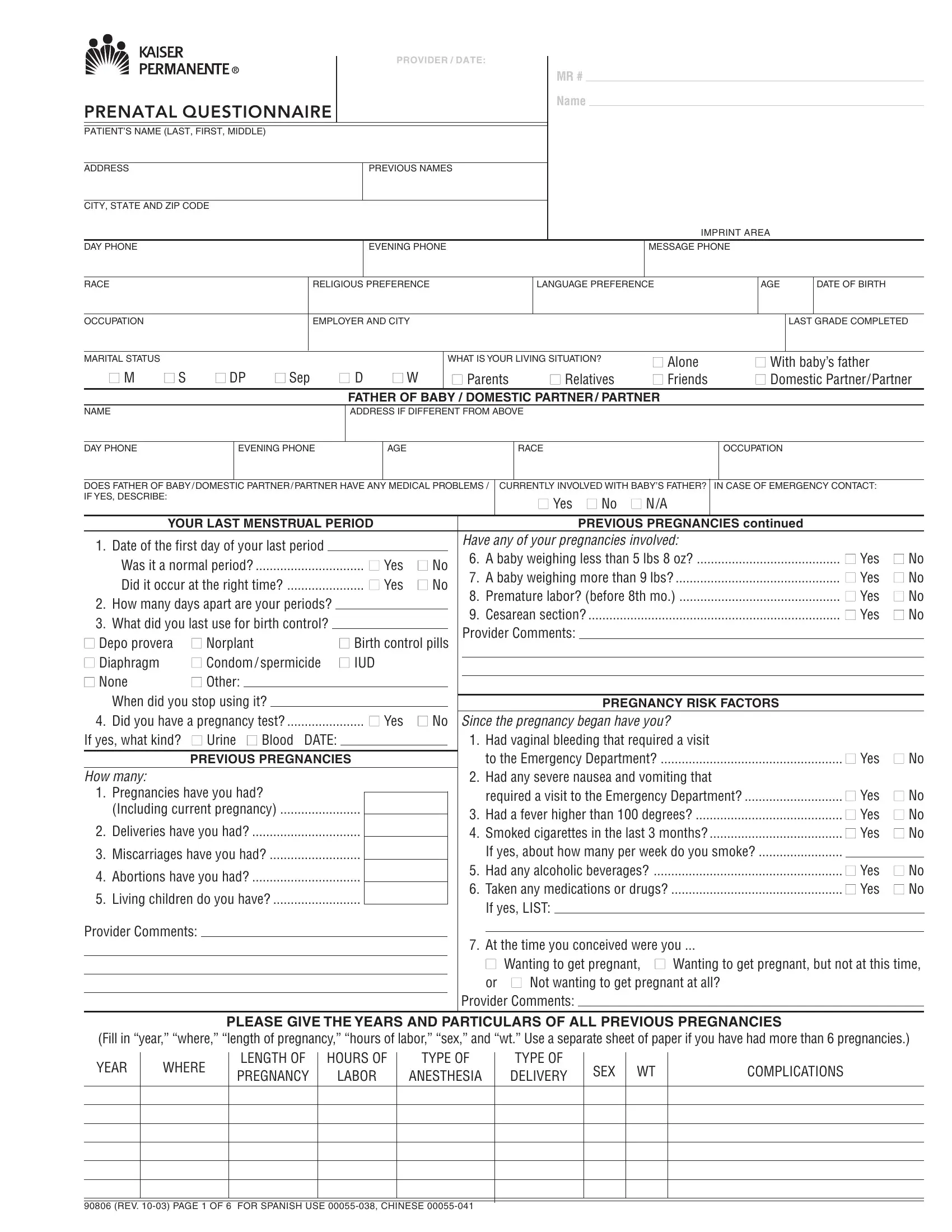
Are you expecting a baby soon? Or thinking of starting a family? Knowing what to expect and how to prepare is essential for any mom-to-be. One key step in the pre-natal process is filling out a Kaiser Prenatal Questionnaire Form (KPQ); this form helps providers learn more about your current health, lifestyle decisions, and plans for pregnancy before meeting with you. With the help of this information, medical professionals can create personalized care plans tailored to your individual needs. Keep reading below as we discuss everything from what's included in KPQ forms, why they're important during pre-natal visits, and tips on filing them out correctly.
| Question | Answer |
|---|---|
| Form Name | Kaiser Prenatal Questionnaire Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | prenatal depresssion standard questionnar, prenatal questionnaire s, prenatal questionnaire phone, non invasive prenatal test questionnaire |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PROVIDER / DATE: |
|
|
|
MR # |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
PRENATAL QUESTIONNAIRE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAME |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PATIENT’S NAME (LAST, FIRST, MIDDLE) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
PREVIOUS NAMES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
CITY, STATE AND ZIP CODE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IMPRINT AREA |
|
|
|
|
||||
DAY PHONE |
|
|
|
|
|
|
|
|
|
|
|
|
|
EVENING PHONE |
|
|
|
|
|
|
|
|
|
|
|
|
|
MESSAGE PHONE |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
RACE |
|
|
|
|
|
|
RELIGIOUS PREFERENCE |
|
|
|
|
|
|
LANGUAGE PREFERENCE |
|
|
AGE |
|
DATE OF BIRTH |
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
OCCUPATION |
|
|
|
|
|
|
EMPLOYER AND CITY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST GRADE COMPLETED |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
MARITAL STATUS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
WHAT IS YOUR LIVING SITUATION? |
|
■ Alone |
|
■ With baby’s father |
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
■ M |
■ S |
■ DP |
|
■ Sep |
■ D |
|
■ W |
|
■ Parents |
|
|
■ Relatives |
|
■ Friends |
|
■ Domestic Partner/Partner |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FATHER OF BABY / DOMESTIC PARTNER / PARTNER |
|
|
|
|
|
|
|
||||||||||||||||||||
NAME |
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS IF DIFFERENT FROM ABOVE |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
DAY PHONE |
|
|
EVENING PHONE |
|
|
|
|
AGE |
|
|
|
|
|
|
|
|
RACE |
|
|
|
|
OCCUPATION |
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
DOES FATHER OF BABY / DOMESTIC PARTNER / PARTNER HAVE ANY MEDICAL PROBLEMS / |
CURRENTLY INVOLVED WITH BABY’S FATHER? |
|
IN CASE OF EMERGENCY CONTACT: |
|
|||||||||||||||||||||||||||||||||||||
IF YES, DESCRIBE: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
■ Yes ■ No |
■ N/A |
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
YOUR LAST MENSTRUAL PERIOD |
|
|
|
|
|
|
|
|
|
|
|
PREVIOUS PREGNANCIES CONTINUED |
|
||||||||||||||||||||||||||
1. Date of the first day of your last period |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Have any of your pregnancies involved: |
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. A baby weighing less than 5 lbs 8 oz? |
|
|
|
■ Yes |
■ No |
||||||||||||||||||||||
Was it a normal period? |
|
|
|
■ Yes |
■ No |
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
7. A baby weighing more than 9 lbs? |
|
|
|
■ Yes |
■ No |
|||||||||||||||||||||||||||||||
Did it occur at the right time? |
|
|
|
■ Yes |
■ No |
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
8. Premature labor? (before 8th mo.) |
|
|
|
■ Yes |
■ No |
|||||||||||||||||||||||||||||||
2. How many days apart are your periods? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
9. Cesarean section? |
|
|
|
|
|
|
|
■ Yes |
■ No |
||||||||||||||||||||
3. What did you last use for birth control? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Provider Comments: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
■ Depo provera |
■ Norplant |
■ Birth control pills |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
■ Diaphragm |
|
■ Condom / spermicide |
■ IUD |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
■ None |
|
■ Other: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
When did you stop using it? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PREGNANCY RISK FACTORS |
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
......................4. Did you have a pregnancy test? |
|
|
■ Yes |
■ No |
|
|
Since the pregnancy began have you? |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
If yes, what kind? |
■ Urine |
■ Blood DATE: |
|
|
|
|
|
|
|
|
|
|
|
1. Had vaginal bleeding that required a visit |
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
to the Emergency Department? |
|
|
|
■ Yes |
■ No |
||||||||||||||||||||
|
|
|
PREVIOUS PREGNANCIES |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
How many: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. Had any severe nausea and vomiting that |
|
|
|
|
|
|
|
||||||||||||
1. Pregnancies have you had? |
|
|
|
|
|
|
|
|
|
|
|
required a visit to the Emergency Department? |
|
■ Yes |
■ No |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
(Including current pregnancy) |
|
|
|
|
|
|
|
|
|
|
3. Had a fever higher than 100 degrees? |
|
|
|
|
■ Yes |
■ No |
||||||||||||||||||||||||
2. Deliveries have you had? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
4. Smoked cigarettes in the last 3 months? |
|
|
|
■ Yes |
■ No |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
3. Miscarriages have you had? |
|
|
|
|
|
|
|
|
|
|
If yes, about how many per week do you smoke? |
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
4. Abortions have you had? |
|
|
|
|
|
|
|
|
|
|
|
5. Had any alcoholic beverages? |
|
|
|
■ Yes |
■ No |
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
6. Taken any medications or drugs? |
|
|
|
■ Yes |
■ No |
||||||||||||||||||||||||||
5. Living children do you have? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
If yes, LIST: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Provider Comments:
7. At the time you conceived were you ...
■Wanting to get pregnant, ■ Wanting to get pregnant, but not at this time, or ■ Not wanting to get pregnant at all?
Provider Comments:
PLEASE GIVE THE YEARS AND PARTICULARS OF ALL PREVIOUS PREGNANCIES
(Fill in “year,” “where,” “length of pregnancy,” “hours of labor,” “sex,” and “wt.” Use a separate sheet of paper if you have had more than 6 pregnancies.)
YEAR |
WHERE |
LENGTH OF |
HOURS OF |
TYPE OF |
TYPE OF |
SEX |
WT |
COMPLICATIONS |
|
PREGNANCY |
LABOR |
ANESTHESIA |
DELIVERY |
||||||
|
|
||||||||
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
90806 (REV.
PATIENT NAME
MR#
PHYSICIAN
YOUR MEDICAL HISTORY |
|
Yes |
No |
|
Provider Comments |
|
SOCIAL CIRCUMSTANCES |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Are you allergic to any medications? |
|
|
|
|
1. |
Have you ever sought |
|
|
Yes |
|
No |
|
|
Provider Comments |
|||||||
If yes, LIST: |
|
|
|
|
|
|
|
professional help for |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
an emotional problem? |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
2. |
Is your work or home |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
stressful? |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
3. |
Is your living situation |
|
|
|
|
|
|
|
|
|
|
|||
Do you have or have you ever had: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
unsafe /unstable? |
|
|
|
|
|
|
|
|
|
|
||||
1. |
Abnormal Pap test |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
Are you constantly dieting? |
|
|
|
|
|
|
|
|
||||||||
2. |
Anemia / blood transfusions |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
Do you foresee any problems |
|
|
|
|
|
|
|
|
||||||||
3. |
Arthritis or bone fractures |
|
|
|
|
|
|
|
coming to prenatal checkups? |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
4. |
Asthma |
|
|
|
|
6. |
Do you have any fears about |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
this pregnancy or baby? |
|
|
|
|
|
|
|
|
|
|
||
5. |
Bleeding tendencies |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
7. |
Within the last year - or since |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
6. |
Blood clots in veins or lungs |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
you have been pregnant - |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
7. |
Breast surgery |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
have you been hit, slapped, |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
8. |
Cancer |
|
|
|
|
|
|
|
kicked or otherwise physically |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
hurt by someone? |
|
|
|
|
|
|
|
|
|
|
||
9. |
Chicken pox |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
8. |
Are you in a relationship |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
10. |
Chlamydia |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
with a person who threatens |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
11. |
Diabetes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
or physically hurts you? |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
12. |
Frequent bladder infections |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9. |
Has anyone forced you to |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
13. |
Gall bladder disease |
|
|
|
|
|
|
|
have sexual activities that |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
made you uncomfortable? |
|
|
|
|
|
|
|
|
|
|
||
14. |
Heart disease |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
15. |
Hepatitis |
|
|
|
|
10. |
Are you worried about |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
your partner’s drug or |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
16. |
Herpes (you or your partner) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
alcohol use? |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
17. |
High blood pressure |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
FATHER OF BABY HISTORY (IF APPLICABLE) |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||
18. |
HIV |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Has the father of the baby? |
|
|
|
Yes |
|
No |
DON’T |
Dr. Comments |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
KNOW |
|||||||||
19. |
HPV or genital warts |
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
1. Had any blood transfusions? |
|
|
|
|
|
|
|||||||||
20. |
Kidney stones |
|
|
|
|
|
|
2. Tested positive for HIV? |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
3. Had herpes? |
|
|
|
|
|
|
|
|
|
|
|||
21. |
Lung disease |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
4. Smoked cigarettes? |
|
|
|
|
|
|
|
|
|
|
|||
22. |
Major surgery / hospitalization |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
POSTPARTUM CONTRACEPTION |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||
23. |
Mental illness / depression |
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
24. |
Migraine headaches |
|
|
|
|
|
|
1. Do you plan to begin a birth control |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
25. |
Problems w/ anesthesia |
|
|
|
|
|
|
|
method after your baby is born? .................................. ■ Yes ■ No |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
26. |
Problems getting pregnant/infertility |
|
|
|
|
|
|
2. If yes, what will you use? |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
27. |
Seizures/epilepsy |
|
|
|
|
|
|
|
■ Vasectomy |
■ Birth control pills |
■ Diaphragm |
||||||||||
28. |
Syphilis |
|
|
|
|
|
|
|
■ Condom / spermicide |
■ IUD |
|
|
|
|
■ Depo provera |
||||||
29. |
Thyroid problems |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
■ Norplant |
■ Tubal sterilization |
|
||||||||||||
30. |
Tuberculosis |
|
|
|
|
|
|
|
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
FAMILY HISTORY |
|
|
|
|
Provider Comments: |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Has anyone in your family ever had? Yes |
No |
Which family member? |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
1.Asthma?
2.Tuberculosis?
3.Heart disease?
4.Hypertension?
5.Kidney disease?
6.Diabetes?
7.Seizures / epilepsy?
8. |
Sickle cell / thalassemia? |
|
BREAST FEEDING PLAN |
|
|
9. |
Twins? |
|
|
|
|
|
1. Do you plan to breastfeed this baby? |
■ Yes ■ No |
|||
10. |
Birth defects? |
|
|||
|
|
|
|
||
REVIEWED BY |
|
|
DATE |
|
|
|
|
|
Provider Signature |
|
|
SIGNED BY |
|
|
DATE |
|
|
|
|
|
Patient’s Signature |
|
|
|
|
|
|
|
|
90806 (REV.