State of California—Health and Human Services Agency
California Department of Public Health
RENEWAL – PERSONNEL CLINICAL LABORATORY LICENSE/CERTIFICAT
CONTINUING EDUCATION REQUIREMENTS
Each person licensed under Division 2, Chapter 3 of the California Business and Professions Code (BPC), commencing with Section 1200, whose license or certificate is in active status must complete the required continuing education hours.
At the time of renewal, you must provide the Department with the date of issue on certificate, California approved accrediting agency number (AA number) and name, program title, course number, and number of contact hours received for each continuing education program you have successfully completed. Please complete and return the Continuing Education Activity Summary (on the back of this page).
NOTE: Submit the renewal application with the CE Activity Summary and renewal fee. The renewal fee can be found on
the following website: https://www.cdph.ca.gov/Programs/OSPHLD/LFS/CDPH%20Document%20Library/A-License-FeeSchedules.pdf
Title 17 of the California Code of Regulations, section 1031.5, requires a license or certificate to be renewed by filing a renewal application at least 60 days prior to the end of the license or certificate period.
Please note: LFS does not accept applications, renewals, or inquiries in person at the Richmond office. Applications must be sent by mail. Inquiries can be submitted by email LFSRenewals@cdph.ca.gov or by telephone (510-620-3800). Applications are processed in the order in which they are received.
CE requirements (California Business and Professions Code section 1260)
•Directors, Cytotechnologists, Clinical Laboratory Scientists, and Medical Laboratory Technicians: O 24 CE hours per 2-year renewal cycle
•Phlebotomists:
O6 CE hours per 2-year renewal cycle
You must retain for a minimum of four years the continuing education documents received from providers approved under the California Code of Regulations, Title 17, section 1038.4. Do not forward such documents to the department unless you are instructed to do so.
A number of renewal applications will be audited by the department each year. A notice will be sent by mail to those who are selected.
Regulations require that you notify this office by email WITHIN 30 DAYS of any change of name or address. Send notification to Laboratory Field Services at LFSRenewals@cdph.ca.gov. Please put “Change of Address” in the subject line.
PLEASE PROVIDE THE FOLLOWING INFORMATION:
Name: ___________________________________________________________________________________________
Daytime telephone number: _______________________ Home telephone number: _____________________________
E-mail address (if available): _________________________________________________________________________
Laboratory Field Services
(510)620-3800 ● (510) 620-3692 FAX ● LFSRenewals@cdph.ca.gov Internet Address: www.cdph.ca.gov/lfs
LAB 177 A (revised 3/16) |
Page 1 of 2 |
State of California – Health and Human Services Agency |
California Department of Public Health |
|
Laboratory Field Services |
RENEWAL – CLINICAL LABORATORY PERSONNEL LICENSE/CERTIFICATE
CONTINUING EDUCATION ACTIVITY SUMMARY
Return to: |
California Department of Public Health |
Please write your license or certificate number on your check. |
|
Accounting Section / Cashiering Unit |
|
|
|
|
MS 1601 P. O. Box 997376 |
|
|
|
|
|
Sacramento, CA 95899-7376 |
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
License/Certificate Number |
|
Phone – Daytime |
Phone – Alternate |
|
|
|
|
|
|
Mailing Address (number, street) |
|
City |
|
State |
ZIP Code |
|
|
|
|
|
|
Email address (if available) |
|
|
|
|
|
|
|
|
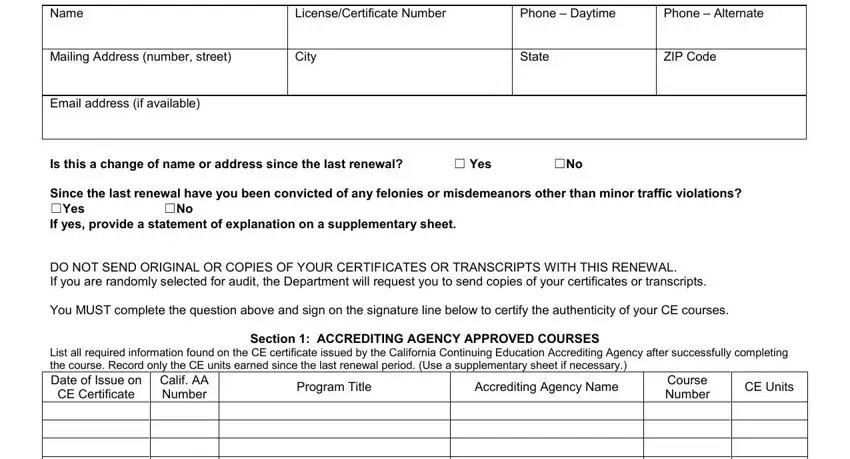
Is this a change of name or address since the last renewal? |
☐ Yes |
☐No |
|
Since the last renewal have you been convicted of any felonies or misdemeanors other than minor traffic violations?
☐Yes ☐No
If yes, provide a statement of explanation on a supplementary sheet.
DO NOT SEND ORIGINAL OR COPIES OF YOUR CERTIFICATES OR TRANSCRIPTS WITH THIS RENEWAL.
If you are randomly selected for audit, the Department will request you to send copies of your certificates or transcripts.
You MUST complete the question above and sign on the signature line below to certify the authenticity of your CE courses.
Section 1: ACCREDITING AGENCY APPROVED COURSES
List all required information found on the CE certificate issued by the California Continuing Education Accrediting Agency after successfully completing the course. Record only the CE units earned since the last renewal period. (Use a supplementary sheet if necessary.)
Date of Issue on |
Calif. AA |
CE Certificate |
Number |
|
|
Section 2: COLLEGE OR UNIVERSITY LEVEL COURSES
List all successfully completed accredited college or university courses relevant to clinical laboratory science scope of practice since the last renewal period. (Use a supplementary sheet if necessary.)
I attest that I have taken the current courses listed above and have certificates in my possession to verify successful completion of the continuing education courses listed in Section 1 or an official transcript for the courses from an accredited college or university listed in Section 2. I understand that I am responsible for maintaining these legal documents for four years.
Warning: Failure to provide complete information may result in delay in processing your license/certification renewal.
Signature: __________________________________________________ |
Date: ______________________________ |
|
|
Laboratory Field Services
(510)620-3800 ● (510) 620-3692 FAX ● LFSRenewals@cdph.ca.gov Internet Address: www.cdph.ca.gov/lfs
LAB 177 B (revised 3/16) |
Page 2 of 2 |