The Larc Program Hospital Jamaica form serves as a crucial gateway for individuals seeking specialized treatment at the intersection of HIV/AIDS and substance abuse. This intensive residential program, updated in November 2011, positions itself as more than just a recovery facility; it's a comprehensive ecosystem designed to offer stabilization, case management, and housing search services within a 90-day framework. Tailored to meet the nuanced needs of each participant, LARC aims to provide a safe and structured environment conducive to recovery and wellness. Eligibility for the program is detailed and comprehensive, ensuring a fit between the services offered and the needs of potential participants. Criteria include a documented history of alcoholism or drug addiction, medical stability, and HIV infection, among others. The program emphasizes inclusivity, integrating persons undergoing methadone treatment and offering a range of counseling and training programs. Located within the Lemuel Shattuck Hospital, it boasts necessary facilities and accessibility features, suggesting a thoughtful consideration of its resident's needs. Application processes involve several steps, from phone screenings to in-person interviews, each designed to thoroughly evaluate and prepare applicants for what lies ahead. The form also underscores the importance of consent and communication between care providers, highlighting a collaborative approach to recovery. Through its detailed forms and structured process, LARC exhibits a comprehensive strategy aimed at addressing the complexities of addiction recovery amidst the challenges of living with HIV/AIDS.
| Question | Answer |
|---|---|
| Form Name | Larc Program Hospital Jamaica Form |
| Form Length | 14 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 3 min 30 sec |
| Other names | Joelyn, Portis, 2011, HPRP |

!"!#$%&'
()
*"
+*",
!
"/
"/0
"
1
/
/
/
)1
)1
*"!
*21
(!4&67&
8935%66:6;79
<8935%66:7=%
8...515
Updated 11.2011
The !!"# (LARC) is an intensive residential program which offers comprehensive substance abuse stabilization and case management/housing search services for up to 90 days. Such services are provided within a treatment'planning model that is individualized to meet the unique needs of each client. In this way, LARC offers a safe and structured space in which program participants can focus on establishing or re' establishing rituals of recovery and wellness that enhance quality of life.
LARC serves men and women living with HIV/AIDS and alcoholism and/or drug addiction whose histories of addiction relapse have jeopardized their ability to access and/or maintain stable residency in either treatment or housing programs. LARC fully integrates persons involved in methadone treatment into the stabilization program.
Individual Addiction/Relapse Prevention Counseling
Group Counseling (over 30 groups weekly)
Comprehensive Case Management
Housing Search Counseling and Advocacy
Stress Reduction Trainings
Life Skills Building, Medication Management and Stress Reduction Techniques
18 years of age or older
History of alcoholism and/or drug addiction with recent instability/relapse
HIV infection
Medical clearance for inpatient substance abuse treatment (detoxification from all illegal and/or unprescribed substances)
Medical, psychiatric and neurologic stability with the ability to engage in the program
Non'infectious tuberculosis status
LARC is located on the 11th floor (north) of the Lemuel Shattuck Hospital in Jamaica Plain. The hospital building itself is situated on the edge of Franklin Park within walking distance of the Forest Hills Orange Line T Station.
The LARC program has 20 comfortable private and semi'private beds, 4 spacious bathrooms, an ample kitchen and dining area, a large solarium/group room, and several staff office spaces. In addition, LARC has laundry facilities which include clothes washers and dryers. The LARC program is handicapped accessible.

!"!#$%&'
()
*"
+*",
!
"/
"/0
"
1
/
/
/
)1
)1
*"!
*21
(!4&67&
8935%66:6;79
<8935%66:7=%
8...515
Updated 11.2011
$$
To be eligible for admission, an applicant !"%#& documentation of the following:
1.A history of alcoholism and/or drug addiction
2.Medically, Psychiatrically and Neurologically able to participate in an intense treatment program
3.HIV infection, including CD4 count and Viral Load Number (within last 4 months)
4.Medical clearance for inpatient treatment (detoxed from all illegal and unprescribed substances)
5.Recent instability in her/his addiction recovery (relapse or risk of relapse)
6.Verification of Financial Resources and Expenses
In order for the application to proceed, all release formsneed to be signed allowing the clinical staff of Victory Programs Living and Recovering Community (LARC) to communicate with their primary care physician, mental health provider(s), methadone provider, and any other relevant care providers.
$
Phone Screening
An initial phone screen is conducted to insure that the applicant meets the eligibility criteria.
Document Completion
The identified provider coordinates the completion and return of required forms and the submission of appropriate documentation, including:
Program Application Form.
Physician’s Referral Form.
Applicant’s Consent to the Release of Information Form(s)
Financial Resources and Expenses Verification Documentation
Methadone Provider’s Referral Form (if applicable)
Face to Face Interview
The applicant comes to LARC for an interview with program staff. This interview includes:
The initial intake assessment
Signing of necessary releases to continue the intake process
Signing of the Client Agreement to Program Participation and the Client Agreement to Rights and Responsibilities
Program Acceptance
>111?*"@.?15
6 |

!"!#$%&'
()
*"
+*",
!
"/
"/0
"
1
/
/
/
)1
)1
*"!
*21
(!4&67&
8935%66:6;79
<8935%66:7=%
8...515
Updated 11.2011
'#(%%###)'%**!#
I, ________________________________________, authorize the staff of the
referring program __________________________________________________,
and the staff of The Living And Recovering Community (LARC) to exchange any
information regarding my addiction, health care, and case management needs and
resources that may be useful in facilitating my application and possible admission to
the LARC program. I understand that my records are protected under the federal
regulation governing Confidentiality of Alcohol and Drug Abuse Patient Records, 42
CFR Part 2, and the Health Insurance Portability and Accountability Act of 1996
(“HIPPA”), 45 C.F.R. Pts. 160 & 164, and cannot be disclosed without my written
consent unless otherwise provided for in the regulations. I also understand that I
may revoke this consent at any time except to the extent that action has been taken
in reliance on it, and that in the event this consent expires one year from its
execution or upon the withdrawal of my application or my discharge from the LARC
program.
_____________________________ |
________________________ |
Signature of Client |
Date |
_____________________________ |
________________________ |
Signature of Witness |
Date |
7 |

!"!#$%&'
()
*"
+*",
!
"/
"/0
"
1
/
/
/
)1
)1
*"!
*21
(!4&67&
8935%66:6;79
<8935%66:7=%
8...515
Updated 11.2011
*(%!
$
Applicant’s name: _____________________________________________________
Current address:_______________________________________________________
Telephone #: _________________________________________________________
Age: ________ Date of birth: _________ Gender: _________ Pregnant (Y/N) _____
SS#: ________________________________ Language(s) spoken: ______________
Has the applicant participated in the LARC program before? ________ When? _____
$
Name of referring provider: _____________________________________________
Relationship to applicant: _______________________________________________
Agency: _____________________________________________________________
Address:_____________________________________________________________
Phone: ___________________________________ Fax:_______________________
Provider’s signature and date:____________________________________________
Reasons for LARC Referral: _____________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
+
Description of applicant’s most recent addiction relapse: ______________________
____________________________________________________________________
Description of applicant’s current recovery status:____________________________
____________________________________________________________________
Description of current alcohol/ drug usage (if applicable): ______________________
____________________________________________________________________
Description of applicant’s detoxification needs: ______________________________
Is the applicant involved in methadone treatment? Yes___ No: ___ Dosage: ______
Methadone provider agency name and #: ___________________________________
= |

!"!#$%&'
()
*"
+*",
!
"/
"/0
"
1
/
/
/
)1
)1
*"!
*21
(!4&67&
8935%66:6;79
<8935%66:7=%
8...515
Updated 11.2011
$$
Name of primary care physician: _________________________________________
Physician’s phone number: ______________________________________________
Other involved health care agencies (CMA, VNA,I)?: _______________________
Date of HIV diagnosis: _________________________________________________
Opportunistic infections and dates: ________________________________________
____________________________________________________________________
Does applicant have any neurological involvement related to HIV? Please describe:
____________________________________________________________________
____________________________________________________________________
Current medications: __________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
Current medical status: _________________________________________________
____________________________________________________________________
$
What is the applicant current housing situation?______________________________
____________________________________________________________________
Is applicant’s current housing situation safe? ________________________________
____________________________________________________________________
What are the applicant’s housing needs? ___________________________________
____________________________________________________________________
Amount of monthly rental payment (if applicable): ___________________________
$$
Is applicant currently seeing mental health care provider? Yes____ No____
How frequently? ________________________ Date of last visit:________________
Mental health care provider’s name: _______________________________________
Mental health provider’s phone #:_________________________________________
% |

!"!#$%&'
()
*"
+*",
!
"/
"/0
"
1
/
/
/
)1
)1
*"!
*21
(!4&67&
8935%66:6;79
<8935%66:7=%
8...515
Updated 11.2011
Psychiatric history (include diagnosis and type of treatment):
__________________________________________________________________________
__________________________________________________________________________
$$$
What are the applicant’s immediate case management needs?
__________________________________________________________________________
__________________________________________________________________________
What workers/ agencies are providing case management support to the applicant at present?
__________________________________________________________________________
__________________________________________________________________________
Does the applicant have legal cases pending, and if so, what is the current status of these legal issues?
__________________________________________________________________________
__________________________________________________________________________
$
Applicant’s total current monthly household income: _______________________________
Current sources of income (include employment, benefits, food stamps, other sources):
__________________________________________________________________________
Medicaid number and type: ___________________________________________________
Recipient identification number (if applicable): ____________________________________
Other Insurance (CMA, NHP, HCHP)? __________________________________________
Married: ____ Unmarried: _____ Divorced: _____ Widowed: _____ Couple: _____
Name of significant other (if applicable): _________________________________________
Does applicant have children, and if so, how many?________________________________
Describe applicant’s “family” and/or system of support: _____________________________
__________________________________________________________________________
Describe presence of addiction in applicant’s family? ______________________________
__________________________________________________________________________
__________________________________________________________________________
__________________________________________________________________________
9 |
!"!#$%&'
()
*"
+*",
!
"/
"/0
"
1
/
/
/
)1
)1
*"!
*21
(!4&67&
8935%66:6;79
<8935%66:7=%
8...515
Updated 11.2011
|
#$"#!%$"# |
|||
# $&" ' %($ ) |
||||
|
|
|
|
|
%$*#*"'#* |
||||
! $& "$"# |
||||
$)!* |
||||
|
|
|
||
,"%#*)
___________________________ |
_______________________________ |
Name of Client |
Client’s Date of Birth |
___________________________ |
_______________________________ |
Name of Primary Care Physician |
Physician’s Phone Number |
!"
I, ____________________________, authorize my physician,________________________,
to disclose to LARC the information requested on this form to assist in my admission to and participation in the LARC program. I understand that my records are protected under the federal regulations governing Confidentiality of Alcohol and drug Abuse Patient Records, 42 CFR Part 2, and cannot be disclosed without my written consent unless otherwise provided for in the regulations. I also understand that I may revoke this consent at any time except to the extent that action has been taken in reliance on it, and that in any event this consent expires one year from its executions or upon the withdrawal of my application or my discharge from the LARC program.
______________________________ |
________________________________ |
Signature Client |
Signature of Witness |
+(
I, __________________________________________ (please print name), am currently
providing medical care for ______________________________________________ at the
following clinic/hospital, __________________________________________. As such, I
certify that he/she;
a diagnosis of AIDS
is HIV symptomatic
is HIV asymptomatic
$
The following blood counts, indicated below, have been taken within the last four months;
."# |
' |
#*/0 |
|||
|
|
|
|
|
|
|
|
|
|
|
AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAAAAAAAAAAAAAAAA |
|
|
|
! |
|
|
|
3 |
||
!"!#$%&'
()
*"
+*",
!
"/
"/0
"
1
/
/
/
)1
)1
*"!
*21
(!4&67&
8935%66:6;79
<8935%66:7=%
8...515
Updated 11.2011
#$"#!%$"# |
|||||
# $&" ' %($ ) |
|||||
|
|
|
|
|
|
%$*#*"'#* |
|||||
|
|
|
|
||
! $& "$"# |
|||||
$)!* |
|||||
|
|||||
$$$$
The applicant, ___________________________________, is currently on the following
medication regimen. Please complete the below list accurately or attach a copy of the applicant’s current medication list. For this application to be processed further, an applicant
must have a 12 %"&&' *!# should he/she be admitted to the program.
"#$%#!&
|
Medication Name |
Dosage |
Frequency |
|
|||
|
AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAAAAAA |
|
AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAAAAAA |
|
AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAAAAAA |
|
AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAAAAAA |
|
AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAAAAAA |
|
|
||
|
|
|
|
|
|
||
'& |
|
|
|
|
|
||
|
Medication Name |
Dosage |
Frequency |
|
|||
|
AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAAAAAA |
|
AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAAAAAA |
|
AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAAAAAA |
|
AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAAAAAA |
|
AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAAAAAA |
|
AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAAAAAA |
|
AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAAAAAA |
|
AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAAAAAA |
|
AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAAAAAA |
|
AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAA |
AAAAAAAAAAAAAAAAAAAA |
|
|
||
|
|
|
|
|
|
||
|
|
||
Tuberculosis Assessment is attached to this application
Additional TB information is attached to this application
B |
Client Name:
Today’s Date:
#$"#!%$"# # $&" ' %($ ) %$*#*"'#* ! $& "$"# $)!*
$$
_______________________________
_______________________________
!"!#$%&'
()
*"
+*",
!
"/
"/0
"
1
/
/
/
)1
)1
*"!
*21
(!4&67&
8935%66:6;79
<8935%66:7=%
8...515
Updated 11.2011
The following over'the counter medications are permissible to use as indicated per manufacturer’s recommendations on a PRN basis only and will not conflict with the client’s current medication regimen. The medication doses are not to exceed the manufacturer’s daily recommended dosages:
Acetaminophen
Ibuprofen
Naproxen
Aspirin
Tums/Rolaids
Other: ____________________________
Provider’s Name: __________________________________________
Provider’s Phone: __________________________________________
Provider’s Signature: __________________________________________
; |

!"!#$%&'
()
*"
+*",
!
"/
"/0
"
1
/
/
/
)1
)1
*"!
*21
(!4&67&
8935%66:6;79
<8935%66:7=%
8...515
Updated 11.2011
|
#$ ! %$&*# |
|
"#$ "#!%$"# |
||
# $&" ' %($ ) |
||
%$* #* "'#* |
||
! $& "$"# $ |
||
)!* |
||
|
||
$#)(%*'! |
||
___________________________________ |
__________________________ |
|
Name of Client |
Client’s Date of Birth |
|
___________________________________ |
__________________________ |
|
Methadone Provider Agency |
Staff Contact |
|
___________________________________ |
___________________________ |
|
Mailing Address |
City, State and Zip Code |
|
___________________________________ |
___________________________ |
|
Date of Client’s Entry into Methadone Program |
Telephone Number |
|
'#(%%###)'%**!#
I, ________________________________________________________, authorize the above
agency, _____________________________________________, to disclose to LARC the
information requested on this form to assist in my admission to and participation in the LARC program. I understand that my records are protected under the Federal Regulations governing Confidentiality of Alcohol and Drug Abuse Records, 42 CFR Part 2 and cannot be disclosed without my written consent unless otherwise provided for in the regulations. I also understand that I may revoke this consent at any time except to the extent that it has been taken in reliance on it, and that in any event this consent expires one years from it’s execution or upon withdrawal of my application or my discharge from the LARC program.
_______________________________________ |
_____________________________ |
Signature of Client |
Date |
$#)(%*!#
Briefly describe the applicant’s dosage history: ______________________________________
_____________________________________________________________________________
_____________________________________________________________________________
Briefly describe the client’s methadone treatment goal (i.e., detox or maintenance)
_____________________________________________________________________________
_____________________________________________________________________________
Documentation of most recent six urine toxicology screens:
Date |
Results |
_______________ |
______________________________________________ |
_______________ |
______________________________________________ |
_______________ |
______________________________________________ |
_______________ |
______________________________________________ |
_______________ |
______________________________________________ |
_______________ |
______________________________________________ |
Methadone Provider Staff Signature_________________________________________ |
|
& |
$#)*#!#
#$ ! %$&*# "#$ "#!%$"# # $&" ' %($ ) %$* #* "'#* ! $& "$"# $ )!*
!"!#$%&'
()
*"
+*",
!
"/
"/0
"
1
/
/
/
)1
)1
*"!
*21
(!4&67&
8935%66:6;79
<8935%66:7=%
8...515
Updated 11.2011
Client Name: _________________________________ Date of Birth: _______________
Home Methadone Clinic: ___________________________________________________
Home Methadone Clinic Fax Number++++++++++++++++++++++++++++++++++++++++
Home Methadone Contact Person: ___________________________________________
Home Clinic Phone Number: ________________________________________________
This is an agreement between the Living and Recovering Community (LARC) of Victory Programs, the client listed above, and his or her home methadone clinic listed above. While at LARC, the client is courtesy dosed at the Methadone Assessment and Treatment (MAT) of Roxbury Comprehensive Community Health Center, located at the Lemuel Shattuck Hospital in Jamaica Plain, the same building in which LARC is located. Upon discharge from LARC the MAT Program ceases courtesy dosing for the LARC client, and the client must return to his or her home clinic for continued dosing.
This is an agreement that, _________________________________________________,
(client name)
will resume services at his or her home clinic, _________________________________,
(home clinic name)
after discharge from the LARC Program. The home clinic will be notified when the client is discharged from LARC by staff of the LARC program and/or the MAT Program. Further arrangements to coordinate care can be made by contacting LARC.
Client Signature: ____________________________________________ Date: ________
Home Clinic Staff Signature: __________________________________ Date: ________
LARC Staff Signature: _______________________________________ Date: ________
!"!#$%&'
()
*"
+*",
!
"/
"/0
"
1
/
/
/
)1
)1
*"!
*21
(!4&67&
8935%66:6;79
<8935%66:7=%
8...515
Updated 11.2011
Clients who are admitted to LARC should bring the following items:
Casual day time clothes, pajamas and a robe
It is suggested that valuables not be brought into the program
Toiletry items, shampoo, toothpaste, etc.
Towels, washrags, etc.
Small alarm clock
Comfortable shoes
Comforter and your own pillow
Insurance card/picture ID
Money to purchase small items
Small radios (televisions are not permitted)
Cell Phone (policies will be explained during intake)
Laundry facilities are available on the floor, but you need to bring your own laundry detergent as each new admission is required to wash his or her clothing upon admission.
As this is a coed program, clients are not expected to wear clothing that is sexually provocative or explicit. All shorts must be of appropriate length and undergarments must be worn at all times. Pajamas are not permitted to be worn to groups, on the floor after morning wake up routine or outside during fresh air breaks. Any clothing with references to drugs, alcohol, tobacco or gambling are not permitted. Shirts and shoes should be worn at all times for sanitary reasons.
6 |
!"!#$%&'
()
*"
+*",
!
"/
"/0
"
1
/
/
/
)1
)1
*"!
*21
(!4&67&
8935%66:6;79
<8935%66:7=%
8...515
Updated 11.2011
7 |

!"!#$%&'
()
*"
+*",
!
"/
"/0
"
1
/
/
/
)1
)1
*"!
*21
(!4&67&
8935%66:6;79
<8935%66:7=%
8...515
Updated 11.2011
FINAL3CHECKLIST FOR PROVIDERS/REFERRAL SOURCES
()((&
Please fax this packet back to 617'522'1345 Attn: Don Drake, PD
4567899751.8 Attn: Don Drake
Please be sure that all paperwork is fully completed, especially the following itemsPlea easbetheysuremayth t allcausepaperworkdelayis infullythecompleted,intake process:especially the following items as they may delay the intake process:
[ ] The HIV Certification is completed by the applicant’s medical provider along with the most recent CD4 count and Viral Load Count
[ ] The HIV certification is completed along with the
current CD4
[ ] The applicant/client is discharged with 30 days of medication. If you and Viral Load counts and signed by the physician
would like to call in the medication, LARC uses the following pharmacy:
[ ] The client is discharged with 30 days worth on medication. If you would like
$+:82;768.7;;6;*&%/% to call that medication in, the pharmacy that LARC uses is:
Note:)!On Friday admissions,7508'754'8878medicationsfor prescribersmay not be delivered until late Monday afternoon so please take this into account when planning weekend medication coverage Note:for theAdmissionsclient. on
Friday may not have their medication
[ ] Is the over the counter medicationdeliveredpermission sheet reviewed and until Monday. Please
completed by the client’s prescriber. Not completing this may limit the take this into consideration when
client’s ability to use over the counter medications. planning
medication coverage for
[ ] If the client is using methadone assisted treatment, are al forms the client.
completed per instructions?
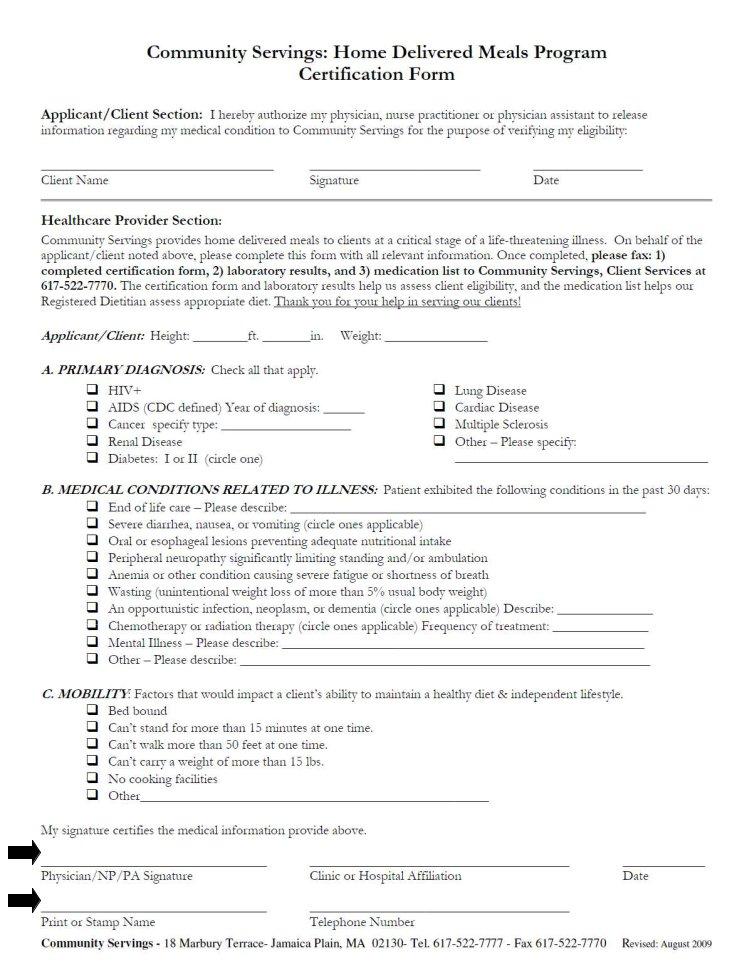
[] Clients at LARC participate in the Community Servings Meal Program.
] Is the over the counter medication sheet reviewed and signed by the
Pleasem dicalbeprovidsurer?that &51, the Home Delivered Meals Program sheet for Community Servings is completed and signed / #)!' &<=%#=)%#"%<
[ ] If the client is using methadone assisted treatment, are all the forms completed per instructions?
[ ] Client is aware of what items he/she are required to bring to the program. Please notify the program ahead of time if the client does not
have access to some of the items.
[ ] Clients at LARC participate in the Community Servings Meal Program.
Please be sure that &51, the Home Delivered Meals Program for
[ ] Cell phones are permitted but can be used in the privacy of the room Community Servings, is completed and signed by the medical providers. only.
LARC staff will complete the Community Servings Packet and fax over lab results and medication list.
If you need anything or have any questions, please do not hesitate to contact us at 617'522'2936. Thank you.
[ ] Client is aware of what items he/she are to bring to the program.
= |