
When you intend to fill out lact form, you won't have to download any software - simply use our PDF tool. FormsPal team is constantly working to enhance the editor and help it become even easier for users with its extensive functions. Bring your experience to a higher level with continually growing and exciting options available today! It merely requires a couple of basic steps:
Step 1: Just press the "Get Form Button" above on this page to get into our pdf editor. This way, you'll find everything that is needed to fill out your document.
Step 2: When you open the PDF editor, you'll notice the document ready to be filled out. Besides filling out different blanks, it's also possible to do other things with the Document, such as writing custom words, modifying the initial text, inserting images, signing the document, and a lot more.
Be attentive when filling out this document. Ensure that all necessary areas are filled out accurately.
1. Whenever filling in the lact form, make sure to incorporate all of the essential blanks in the relevant form section. This will help to speed up the work, making it possible for your details to be processed fast and properly.
2. The next step would be to fill out these particular blank fields: Dues cover calendar year January, Individual M embership Ë Student, Full tim e student status m ust be, Dues payment Options T Online at, T By phoning Credit Card, Membership Applications new or, LASACT receives this Form, Credit Card information Credit, Billing ZIP Code, and Rev November.
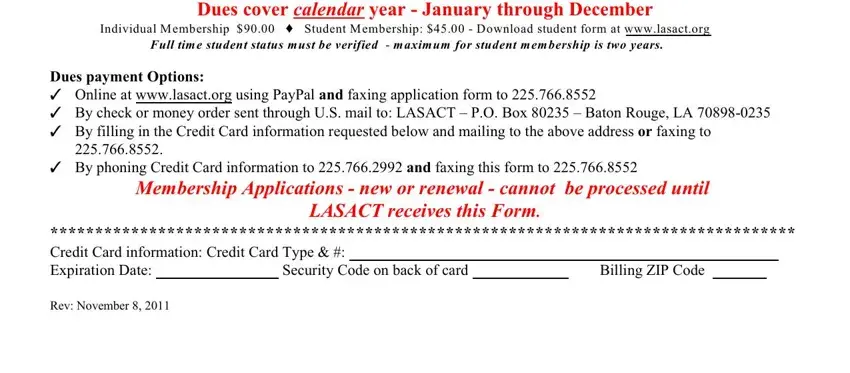
It's easy to make errors while filling in the Membership Applications new or, and so you'll want to take a second look prior to when you submit it.
Step 3: When you've glanced through the information in the document, press "Done" to conclude your FormsPal process. After registering afree trial account with us, you will be able to download lact form or email it immediately. The file will also be readily available through your personal cabinet with your changes. FormsPal is focused on the confidentiality of our users; we ensure that all personal information put into our tool stays protected.