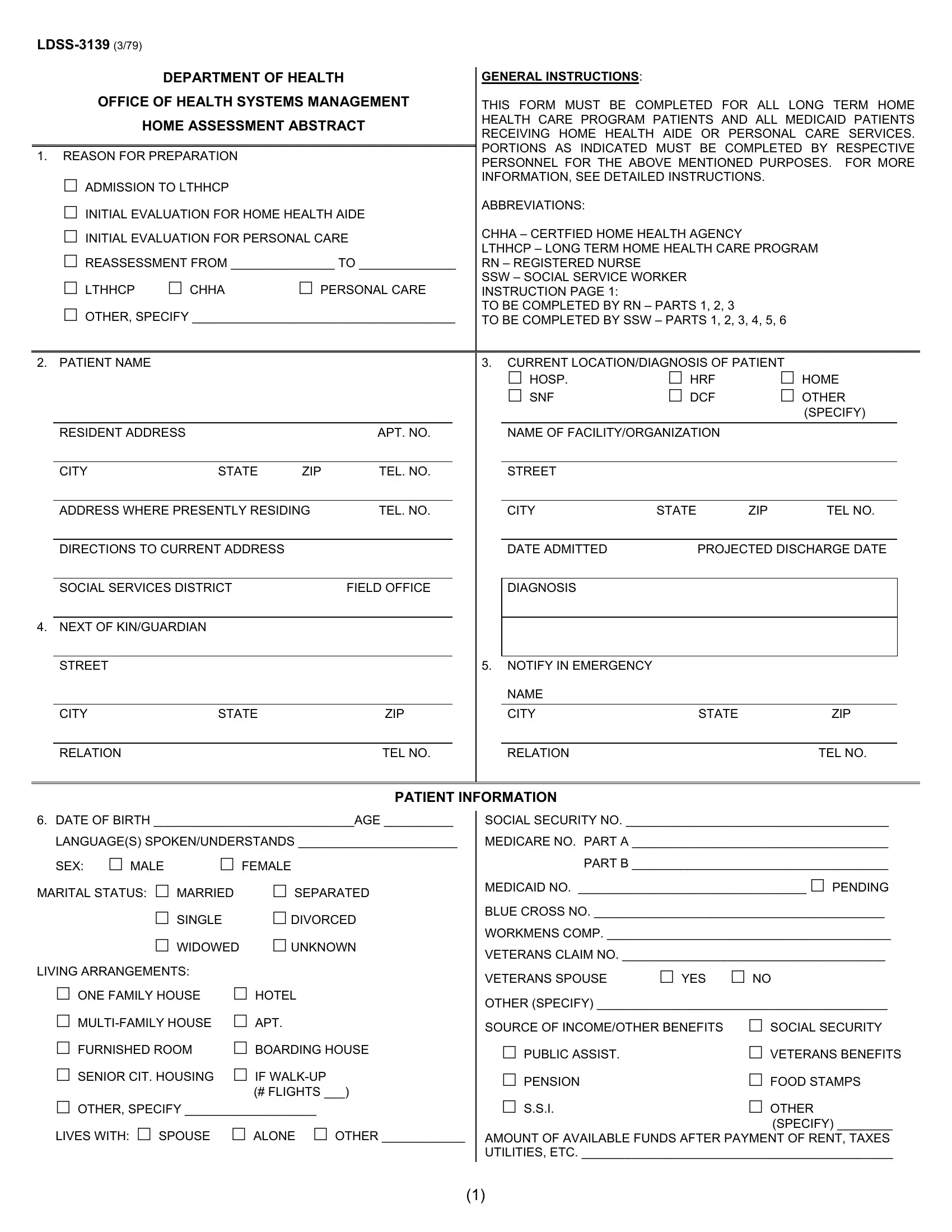
The LDSS-3139 form, issued by the Department of Health Office of Health Systems Management, is a comprehensive document vital for assessing the needs of individuals requiring long-term home health care or Medicaid services related to personal care or home health aide assistance. Its primary use is for admissions into Long Term Home Health Care Programs (LTHHCP), initial evaluations, reassessments, and other specified reasons needing detailed documentation of a patient's situation and care requirements. The form requires collaborative input, typically from registered nurses (RNs) and social service workers (SSWs), covering a wide spectrum of information. This ranges from personal and contact details of the patient, their living arrangements, to the intricate specifics of their health diagnosis, support network, and a meticulous assessment of their home environment's safety and suitability for care delivery. Additionally, it outlines the necessary services, including medical, therapeutic, and support needs, and evaluates the family's capability and willingness to participate in the caregiving process. The goal of this form is to ensure that patients receive appropriate, safe, and coordinated care in their preferred home setting while also detailing the expected recovery outcomes and any significant services that would enable them to live as independently as possible. Furthermore, it includes financial aspects, like the estimation of costs for required services and the source of funding, highlighting its role in planning and facilitating efficient care management for individuals needing long-term home care services.
| Question | Answer |
|---|---|
| Form Name | Ldss 3139 Form |
| Form Length | 6 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 30 sec |
| Other names | ldss 79 get, ldss 3139 from, ldss 3139, home assessment initial |
DEPARTMENT OF HEALTH
OFFICE OF HEALTH SYSTEMS MANAGEMENT
HOME ASSESSMENT ABSTRACT
1.REASON FOR PREPARATION
ADMISSION TO LTHHCP
INITIAL EVALUATION FOR HOME HEALTH AIDE
INITIAL EVALUATION FOR PERSONAL CARE
REASSESSMENT FROM _______________ TO ______________
LTHHCP CHHAPERSONAL CARE
OTHER, SPECIFY ______________________________________
GENERAL INSTRUCTIONS:
THIS FORM MUST BE COMPLETED FOR ALL LONG TERM HOME HEALTH CARE PROGRAM PATIENTS AND ALL MEDICAID PATIENTS RECEIVING HOME HEALTH AIDE OR PERSONAL CARE SERVICES. PORTIONS AS INDICATED MUST BE COMPLETED BY RESPECTIVE PERSONNEL FOR THE ABOVE MENTIONED PURPOSES. FOR MORE INFORMATION, SEE DETAILED INSTRUCTIONS.
ABBREVIATIONS:
CHHA – CERTFIED HOME HEALTH AGENCY
LTHHCP – LONG TERM HOME HEALTH CARE PROGRAM RN – REGISTERED NURSE
SSW – SOCIAL SERVICE WORKER INSTRUCTION PAGE 1:
TO BE COMPLETED BY RN – PARTS 1, 2, 3
TO BE COMPLETED BY SSW – PARTS 1, 2, 3, 4, 5, 6
2. PATIENT NAME
RESIDENT ADDRESS |
|
|
APT. NO. |
|
|
|
|
CITY |
STATE |
ZIP |
TEL. NO. |
|
|
||
ADDRESS WHERE PRESENTLY RESIDING |
TEL. NO. |
||
|
|
|
|
DIRECTIONS TO CURRENT ADDRESS |
|
|
|
|
|
|
|
SOCIAL SERVICES DISTRICT |
|
FIELD OFFICE |
|
4.NEXT OF KIN/GUARDIAN
STREET
CITY |
STATE |
ZIP |
3.CURRENT LOCATION/DIAGNOSIS OF PATIENT
HOSP. |
HRF |
|
HOME |
SNF |
DCF |
|
OTHER |
|
|
|
(SPECIFY) |
|
|
|
|
NAME OF FACILITY/ORGANIZATION |
|
|
|
|
|
|
|
STREET |
|
|
|
|
|
|
|
CITY |
STATE |
ZIP |
TEL NO. |
|
|
||
DATE ADMITTED |
PROJECTED DISCHARGE DATE |
||
|
|
|
|
DIAGNOSIS |
|
|
|
|
|
|
|
|
|
|
|
5.NOTIFY IN EMERGENCY
NAME
CITY |
STATE |
ZIP |
RELATION |
TEL NO. |
RELATION |
TEL NO. |
PATIENT INFORMATION
6.DATE OF BIRTH _____________________________AGE __________
LANGUAGE(S) SPOKEN/UNDERSTANDS _______________________
SEX: |
MALE |
|
FEMALE |
MARITAL STATUS: |
MARRIED |
SEPARATED |
|
|
|
SINGLE |
DIVORCED |
WIDOWED UNKNOWN
LIVING ARRANGEMENTS: |
|
|
|
ONE FAMILY HOUSE |
HOTEL |
|
|
APT. |
|
||
FURNISHED ROOM |
BOARDING HOUSE |
||
SENIOR CIT. HOUSING |
IF |
|
|
|
|
(# FLIGHTS ___) |
|
OTHER, SPECIFY ___________________ |
|
||
LIVES WITH: |
SPOUSE |
ALONE |
OTHER ____________ |
SOCIAL SECURITY NO. ______________________________________
MEDICARE NO. PART A _____________________________________
PART B _____________________________________
MEDICAID NO. _________________________________ |
PENDING |
BLUE CROSS NO. __________________________________________ |
|
WORKMENS COMP. _________________________________________ |
|
VETERANS CLAIM NO. ______________________________________ |
|
VETERANS SPOUSE |
YES |
NO |
OTHER (SPECIFY) __________________________________________ |
||
SOURCE OF INCOME/OTHER BENEFITS |
SOCIAL SECURITY |
|
PUBLIC ASSIST. |
|
VETERANS BENEFITS |
PENSION |
|
FOOD STAMPS |
S.S.I. |
|
OTHER |
|
|
(SPECIFY) ________ |
AMOUNT OF AVAILABLE FUNDS AFTER PAYMENT OF RENT, TAXES UTILITIES, ETC. _____________________________________________
(1)
7. To be completed by S S W
OTHERS IN HOME/HOUSEHOLD: Indicate days/hours that these persons will provide care to patient. If none will assist explain in narrative.
NAME |
Age |
|
|
1.
Relationship
Days/Hours at Home
Days/Hours will Assist
2.
3.
4.
8.To be completed by S S W
SIGNIFICANT OTHERS OUTSIDE OF HOME: Indicate days/hours when persons below will provide care to patient.
Name |
Address |
Age |
Relationship |
|
|
|
|
1.
Days/Hours Assisting
2.
3.
4.
5.
9.To be completed by S S W
COMMUNITY SUPPORT: Indicate organization/persons serving patient at present or has provided a service in the past six (6) months.
Organization
1.
Type of Service
Presently Receiving
Contact Person
Tel No.
2.
3.
4.
10.To be completed by S S W and R.N.
PATIENT TRAITS:
Yes |
No |
?N/A |
If you check No. ?N/A, describe |
Appears self directed and/or independent
Seems to make appropriate decisions
Can recall med routine/recent events
Participates in planning/treatment program
Seems to handle crises well
Accepts diagnosis
Motivated to remain at home
(2)
11. To be completed by S S W and R.N. as appropriate
FAMILY TRAITS: |
|
|
|
|
|
Yes |
No |
? |
|
|
|
|
|
|
a. Is motivated to keep patient home |
|
|
If no, because |
|
|
|
|
|
|
b. Is capable of providing care (physically & emotionally) |
|
|
If no, because |
|
|
|
|
|
|
c. Will keep patient home if not involved with care |
|
|
Because |
|
|
|
|
|
|
d. Will give care if support service given |
|
|
How much |
|
e.Requires instruction to provide care
In what – who will give
12. To be completed by R.N. |
|
|
|
|
||
|
|
|
|
|
|
|
|
Home/Place where care will be provided: |
Yes |
No |
? |
If problem, describe |
|
|
Neighborhood secure/safe |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
Housing adequate in terms of: |
|
|
|
|
|
|
Space |
|
|
|
|
|
|
|
|
|
|
|
|
|
Convenient toilet facilities |
|
|
|
|
|
|
|
|
|
|
|
|
|
Heating adequate and safe |
|
|
|
|
|
|
|
|
|
|
|
|
|
Cooking facilities & refrigerator |
|
|
|
|
|
|
|
|
|
|
|
|
|
Laundry facilities |
|
|
|
|
|
|
|
|
|
|
|
|
|
Tub/shower/hot water |
|
|
|
|
|
|
|
|
|
|
|
|
|
Elevator |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
Telephone accessible & usable |
|
|
|
|
|
|
|
|
|
|
|
|
|
Is patient mobile in house |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Leaky gas, poor wiring, unsafe floors, |
|
Any discernible hazards (please circle) |
|
|
|
steps, other (specify) |
|
|
|
|
|
|
|
|
|
Construction adequate |
|
|
|
|
|
|
|
|
|
|
|
|
|
Excess use of alcohol/drugs by patient/ |
|
|
|
|
|
|
caretaker; smokes carelessly. |
|
|
|
|
|
|
|
|
|
|
|
|
|
Is patient’s safety threatened if alone? |
|
|
|
|
|
|
|
|
|
|
|
|
|
Pets |
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDITIONAL ASSESSMENT FACTORS: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13. To be completed by R.N. |
|
|
RECOVERY POTENTIAL ANTICIPATED |
|
COMMENTS |
Full recovery |
|
|
|
|
|
Recovery with patient management residual |
|
|
|
|
|
Limited recovery managed by others |
|
|
|
|
|
Deterioration |
|
|
|
|
|
(3)
14.To be completed by R.N. – S S W to complete “D” as appropriate
FOR THE PATIENT TO REMAIN AT HOME – SERVICES REQUIRED
|
|
|
WHO WILL PROVIDE |
|
|
|
|
|
|
|
|
SERVICES REQUIRED |
YES |
NO |
TYPE/FREQ/DUR |
AGENCY/FAMILY |
AGENCY FREQUENCY |
|
|
|
|
|
|
A.Bathing Dressing Toileting Admin. Med. Grooming Spoon feeding Exercise/activity/walking Shopping (food/supplies) Meal preparation
Diet Counseling Light housekeeping
Personal laundry/household linens Personal/financial errands Other
B.Nursing Physical Therapy Home Health Aide Speech Pathology Occupational Therapy Personal Care Homemaking Housekeeping Clinic/Physician Other 1.
2.
C.Ramps outside/inside
Grab bars/hallways/bathroom Commode/special bed/wheelchair Cane/walker/crutches
Other
D.Additional Services (Lab, O2, medication) Telephone reassurance Diversion/friendly visitor
Medical social service/counseling Legal/protective services
Financial management/conservatorship Transportation arrangements Transportation attendant
Home delivered meals Structural modification Other
15.To be completed by S S W and R.N
DMS Predictor Score ____________________________________ Override necessary |
|
Yes |
No |
||||
Can patient’s health/safety needs be met through home care now? |
|
|
Yes |
No |
|||
If no, give specific reason why not |
|
|
|
|
|
|
|
Institutional care required now? |
Yes |
No |
If yes, give specific reason why. |
|
|
||
Level of institutional care determined by your professional judgment: |
SNF |
|
HRF |
DCF |
|||
Can the patient be considered at a later time for home care? |
|
Yes |
No |
N/A |
|
||
(4)
16.To be completed by S S W
SUMMARY OF SERVICE REQUIREMENTS
Indicate services required, schedule and charges (allowable charge in area)
|
|
|
Date |
Est. |
Unit |
|
|
Payment by |
|
|
|||
|
|
|
|
|
|
|
|
|
|
||||
Services |
Provided by |
Hrs./Days/Wk. |
Effective |
Dur. |
Cost |
|
MC |
|
MA |
|
Self |
|
Other |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician |
|
|
|
|
|
|
|
|
|
|
|
|
|
Nursing |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Home Health Aide |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physical Therapy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Speech Pathology |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Resp. Therapy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Med. Soc. Work |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Nutritional |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Personal Care |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Homemaking |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Housekeeping |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other (Specify) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Medical Supplies/Medication |
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Medical Equipment |
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Home Delivered Meals |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Transportation |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Additional Services |
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SUBTOTAL
Structural Modification
Other (Specify) 1.
2.
SUBTOTAL
TOTAL COST
(5)
17. To be completed by S S W and R.N.
Person who will relieve in case of emergency
Name |
Address |
Telephone |
Relationship |
Narrative: Use this space to describe aspects of the patients care not adequately covered above.
Assessment completed by:
R.N.
Date Completed
Local DSS Staff
Date Completed
Supervisor DSS
Date
Agency
Telephone No.
District
Telephone No.
District
Telephone No.
Authorization to provide services:
Local DSS Commissioner or Designee |
Date |
(6)