
You'll be able to complete Ldss 3151 Form instantly using our PDFinity® PDF editor. Our tool is consistently developing to provide the very best user experience achievable, and that is thanks to our resolve for continual enhancement and listening closely to testimonials. Getting underway is easy! All that you should do is take the next basic steps directly below:
Step 1: Just press the "Get Form Button" above on this page to see our pdf editor. This way, you'll find everything that is necessary to work with your file.
Step 2: This editor will give you the capability to work with your PDF form in many different ways. Improve it by including your own text, correct original content, and place in a signature - all close at hand!
It will be straightforward to complete the form with our practical tutorial! Here's what you have to do:
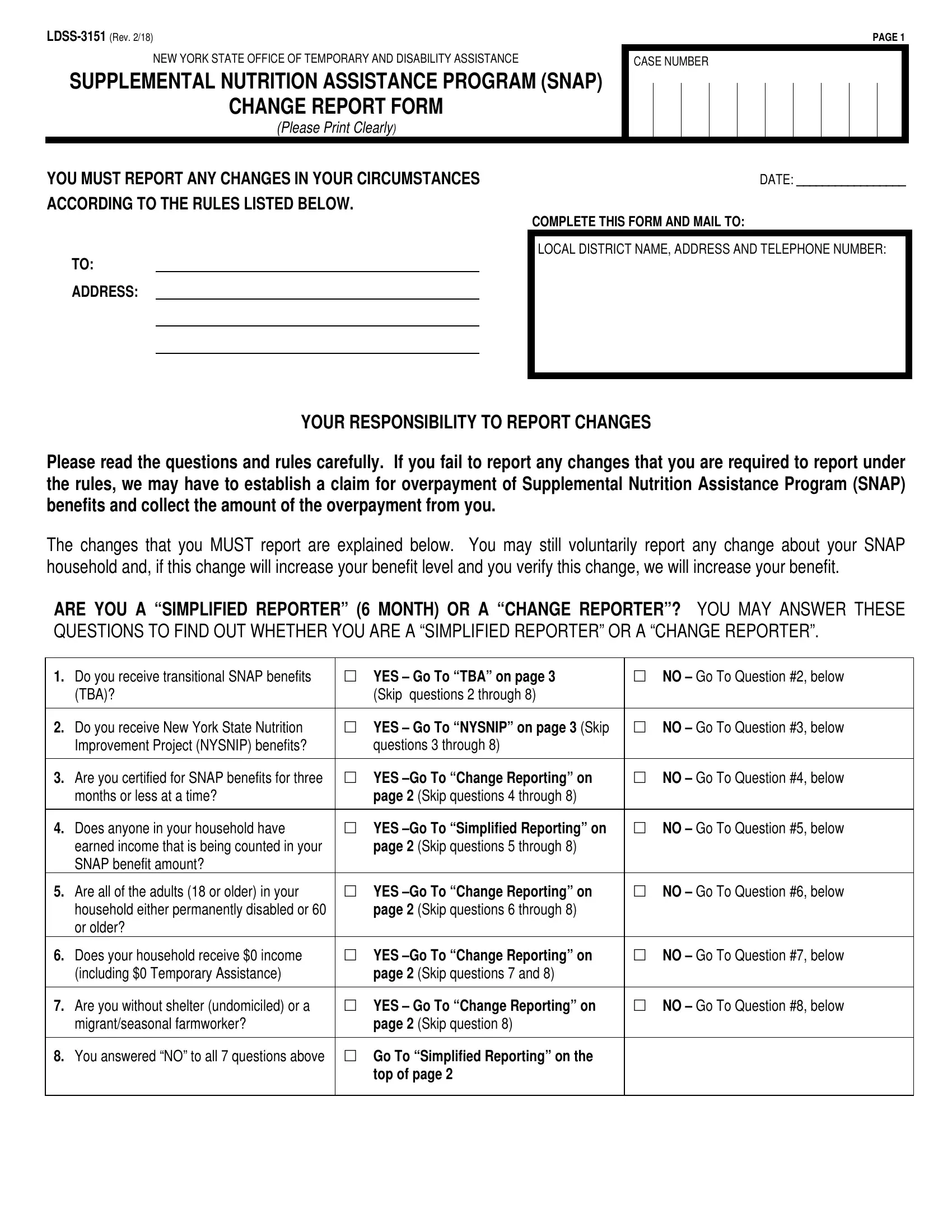
1. Fill out your Ldss 3151 Form with a group of necessary blanks. Gather all the necessary information and make sure nothing is forgotten!
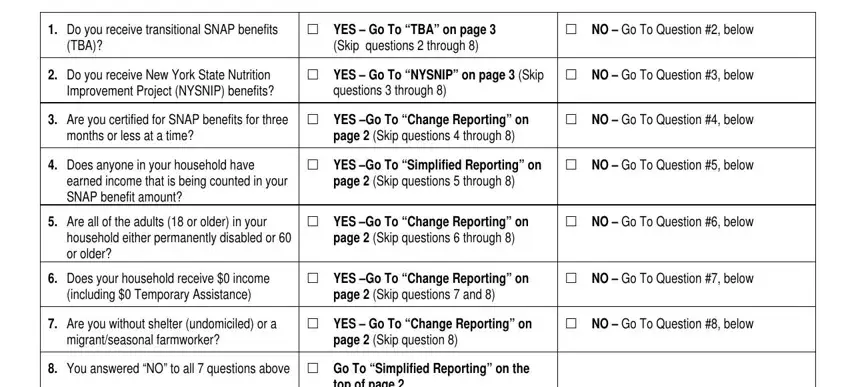
2. Soon after the prior array of blank fields is filled out, go to enter the suitable details in all these: The changes that you MUST report, Do you receive transitional SNAP, TBA, YES Go To TBA on page, Skip questions through, NO Go To Question below, Do you receive New York State, YES Go To NYSNIP on page Skip, NO Go To Question below, questions through, Are you certified for SNAP, YES Go To Change Reporting on, NO Go To Question below, months or less at a time, and page Skip questions through.
3. Completing WITHDRAW FROM SNAP If you no, and IF YOU WITHHOLD INFORMATION ABOUT is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. This next section requires some additional information. Ensure you complete all the necessary fields - SOURCE OF INCOME, WEEK IF WORKING, CHANGE IN HOUSEHOLD List below, NAME, DATE OF, RELATIONSHIP, CHANGE CHECK ONE, DATE, BIRTH, HOW OFTEN RECEIVED, weekly biweekly, monthly, TOTAL NUMBER, OF HOURS, and WORKED PER - to proceed further in your process!
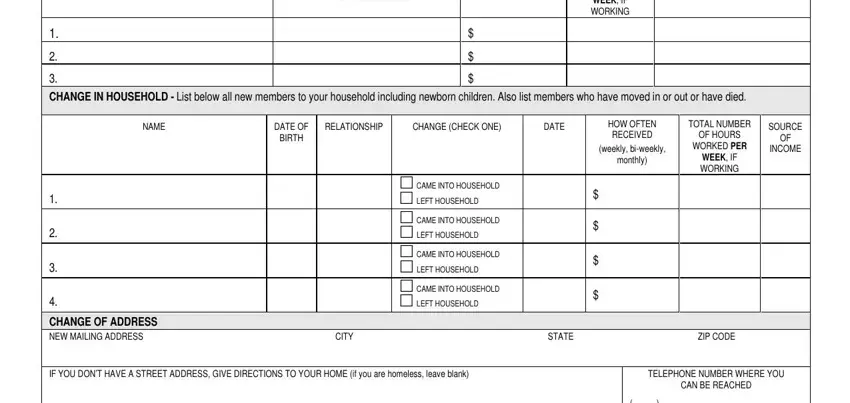
People often make mistakes while completing WORKED PER in this area. You should definitely reread whatever you enter right here.
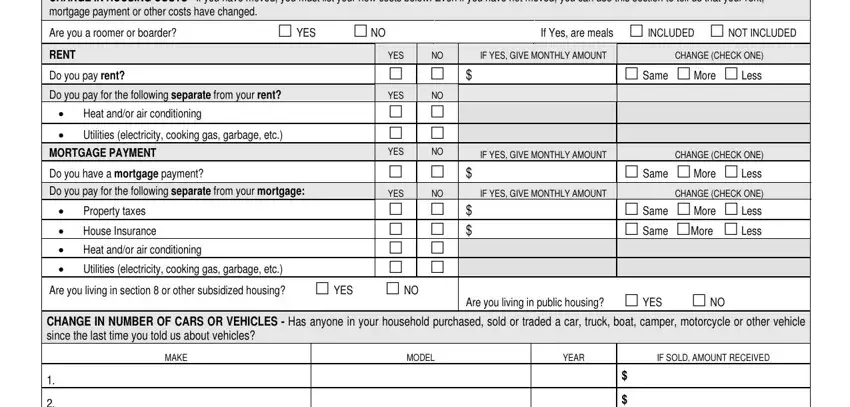
5. Lastly, the following final portion is what you should wrap up before finalizing the PDF. The blanks in this instance include the following: CHANGE IN HOUSING COSTS If you, Are you a roomer or boarder, YES NO, If Yes are meals INCLUDED NOT, RENT, Do you pay rent, Do you pay for the following, Heat andor air conditioning, Utilities electricity cooking gas, MORTGAGE PAYMENT, Do you have a mortgage payment, Do you pay for the following, Property taxes, House Insurance, and Heat andor air conditioning.
Step 3: Check all the information you've entered into the blank fields and then click on the "Done" button. Create a 7-day free trial account at FormsPal and acquire immediate access to Ldss 3151 Form - with all transformations kept and available in your FormsPal account page. FormsPal is dedicated to the confidentiality of our users; we ensure that all personal information handled by our editor stays protected.