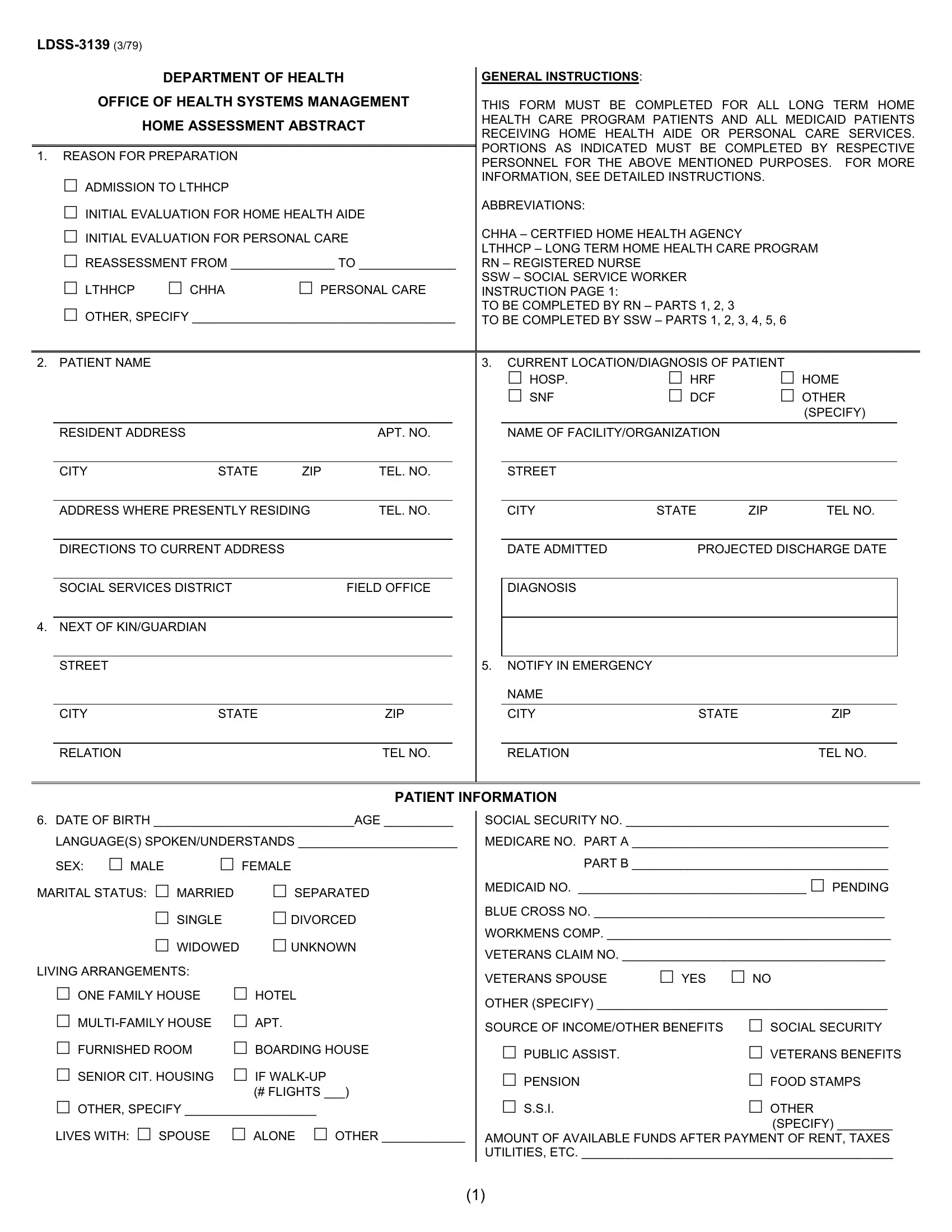
The LDSS-3139 form, issued by the Department of Health Office of Health Systems Management, is a comprehensive document vital for assessing the needs of individuals requiring long-term home health care or Medicaid services related to personal care or home health aide assistance. Its primary use is for admissions into Long Term Home Health Care Programs (LTHHCP), initial evaluations, reassessments, and other specified reasons needing detailed documentation of a patient's situation and care requirements. The form requires collaborative input, typically from registered nurses (RNs) and social service workers (SSWs), covering a wide spectrum of information. This ranges from personal and contact details of the patient, their living arrangements, to the intricate specifics of their health diagnosis, support network, and a meticulous assessment of their home environment's safety and suitability for care delivery. Additionally, it outlines the necessary services, including medical, therapeutic, and support needs, and evaluates the family's capability and willingness to participate in the caregiving process. The goal of this form is to ensure that patients receive appropriate, safe, and coordinated care in their preferred home setting while also detailing the expected recovery outcomes and any significant services that would enable them to live as independently as possible. Furthermore, it includes financial aspects, like the estimation of costs for required services and the source of funding, highlighting its role in planning and facilitating efficient care management for individuals needing long-term home care services.
| Question | Answer |
|---|---|
| Form Name | Ldss 3139 Form |
| Form Length | 6 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 30 sec |
| Other names | ldss 79 get, ldss 3139 from, ldss 3139, home assessment initial |
