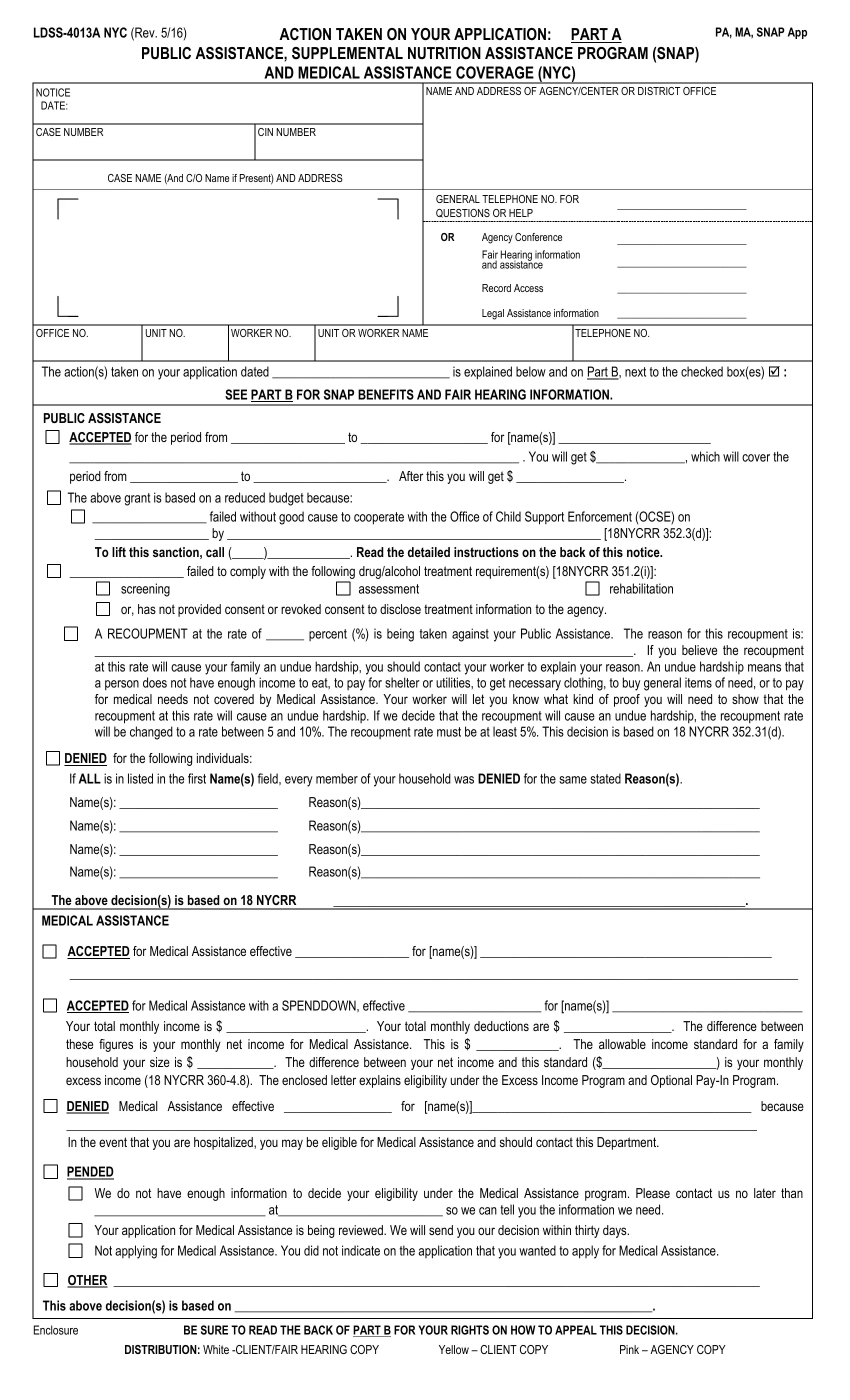
In navigating the complexities of acquiring public assistance, healthcare, and nutritional support, individuals and families often find themselves faced with paperwork that is both crucial and complex. One such document is the LDSS-4013A form, a vital communication from New York City's social services departments regarding the actions taken on applications for Public Assistance, the Supplemental Nutrition Assistance Program (SNAP), and Medical Assistance. Updated in May 2016, this form serves multiple functions. It notifies applicants about the decisions made on their applications—whether accepted, denied, pended, or other actions—and provides the specifics of any public assistance granted, including financial amounts and coverage periods. Crucially, the form details reasons for any denials and directions for appealing decisions, which could range from non-cooperation with child support enforcement to failure to comply with drug and alcohol treatment requirements. The LDSS-4013A form also addresses recoupment rates, indicating the financial adjustments made to assistance payments and offering guidance on how to argue undue hardship. Furthermore, it serves as a doorway to additional resources and rights, including information on family planning services, Child Health Plus coverage for those under 19, and contact details for further assistance. With sections dedicated to notifying applicants of their rights to appeal decisions, request agency conferences, access legal assistance, and more, the LDSS-4013A form epitomizes the intersection of administrative process and the individual's pursuit of assistance, embodying a critical step in navigating the often challenging path to obtaining essential support.
| Question | Answer |
|---|---|
| Form Name | Ldss 4013A Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | w 532 form, form 532, w 532 letter to past or present employer, form w 532 |
ACTION TAKEN ON YOUR APPLICATION: PART A |
PA, MA, SNAP App |
||||
PUBLIC ASSISTANCE, SUPPLEMENTAL NUTRITION ASSISTANCE PROGRAM (SNAP) |
|
||||
|
AND MEDICAL ASSISTANCE COVERAGE (NYC) |
|
|
||
NOTICE |
|
NAME AND ADDRESS OF AGENCY/CENTER OR DISTRICT OFFICE |
|||
DATE: |
|
|
|
|
|
|
|
|
|
|
|
CASE NUMBER |
CIN NUMBER |
|
|
|
|
|
|
|
|
|
|
CASE NAME (And C/O Name if Present) AND ADDRESS |
|
|
|
||
|
|
|
|
|
|
|
|
GENERAL TELEPHONE NO. FOR |
_________________________ |
||
|
|
QUESTIONS OR HELP |
|||
|
|
|
|
||
|
|
OR |
Agency Conference |
_________________________ |
|
|
|
|
Fair Hearing information |
_________________________ |
|
|
|
|
and assistance |
||
|
|
|
Record Access |
_________________________ |
|
|
|
|
Legal Assistance information |
_________________________ |
|
OFFICE NO.
UNIT NO.
WORKER NO.
UNIT OR WORKER NAME
TELEPHONE NO.
The action(s) taken on your application dated ____________________________ is explained below and on Part B, next to the checked box(es) :
SEE PART B FOR SNAP BENEFITS AND FAIR HEARING INFORMATION.
PUBLIC ASSISTANCE
ACCEPTED for the period from __________________ to ____________________ for [name(s)] ________________________
_______________________________________________________________________ . You will get $______________, which will cover the
period from _________________ to _____________________. After this you will get $ _________________.
The above grant is based on a reduced budget because:
__________________ failed without good cause to cooperate with the Office of Child Support Enforcement (OCSE) on
__________________ by ___________________________________________________________ [18NYCRR 352.3(d)]:
To lift this sanction, call (_____)_____________. Read the detailed instructions on the back of this notice.
__________________ failed to comply with the following drug/alcohol treatment requirement(s) [18NYCRR 351.2(i)]:
screening |
assessment |
rehabilitation |
or, has not provided consent or revoked consent to disclose treatment information to the agency. |
|
|
A RECOUPMENT at the rate of ______ percent (%) is being taken against your Public Assistance. The reason for this recoupment is:
_____________________________________________________________________________________. If you believe the recoupment
at this rate will cause your family an undue hardship, you should contact your worker to explain your reason. An undue hardship means that a person does not have enough income to eat, to pay for shelter or utilities, to get necessary clothing, to buy general items of need, or to pay for medical needs not covered by Medical Assistance. Your worker will let you know what kind of proof you will need to show that the recoupment at this rate will cause an undue hardship. If we decide that the recoupment will cause an undue hardship, the recoupment rate will be changed to a rate between 5 and 10%. The recoupment rate must be at least 5%. This decision is based on 18 NYCRR 352.31(d).
DENIED for the following individuals:
If ALL is in listed in the first Name(s) field, every member of your household was DENIED for the same stated Reason(s).
Name(s): _________________________ |
Reason(s)_______________________________________________________________ |
Name(s): _________________________ |
Reason(s)_______________________________________________________________ |
Name(s): _________________________ |
Reason(s)_______________________________________________________________ |
Name(s): _________________________ |
Reason(s)_______________________________________________________________ |
The above decision(s) is based on 18 NYCRR |
_________________________________________________________________. |
MEDICAL ASSISTANCE |
|
ACCEPTED for Medical Assistance effective __________________ for [name(s)] ______________________________________________
___________________________________________________________________________________________________________________
ACCEPTED for Medical Assistance with a SPENDDOWN, effective _____________________ for [name(s)] ______________________________
Your total monthly income is $ ______________________. Your total monthly deductions are $ _________________. The difference between
these figures is your monthly net income for Medical Assistance. This is $ _____________. The allowable income standard for a family
household your size is $ ____________. The difference between your net income and this standard ($__________________) is your monthly
excess income (18 NYCRR
DENIED Medical Assistance effective _________________ for [name(s)]____________________________________________ because
_____________________________________________________________________________________________________________
In the event that you are hospitalized, you may be eligible for Medical Assistance and should contact this Department.
PENDED
We do not have enough information to decide your eligibility under the Medical Assistance program. Please contact us no later than
___________________________ at__________________________ so we can tell you the information we need.
Your application for Medical Assistance is being reviewed. We will send you our decision within thirty days.
Not applying for Medical Assistance. You did not indicate on the application that you wanted to apply for Medical Assistance.
OTHER ______________________________________________________________________________________________________
This above decision(s) is based on __________________________________________________________________.
Enclosure |
BE SURE TO READ THE BACK OF PART B FOR YOUR RIGHTS ON HOW TO APPEAL THIS DECISION. |
||
|
DISTRIBUTION: White |
Yellow – CLIENT COPY |
Pink – AGENCY COPY |
To Lift a Sanction for
A sanction for
the Child Support Enforcement Unit and cooperates.
When __________________ contacts the Child Support Enforcement Unit, he or she will be told what action(s) must be taken to
end the sanction. The sanction will end when he or she takes the required actions(s). If __________________ did not cooperate
but now wants to report a good reason for not cooperating with child support he or she should call (_____)___________________.
Some examples of a good reason for not cooperating with child support are:
∙fear of emotional or physical harm to you or the children in your family; or,
∙the child was born due to rape or incest; or,
∙the child is freed for adoption; or, you are now being assisted by an agency to determine whether to put the child up for adoption and discussions have not gone on for more than three months.
To find out more information about how to end the sanction, call (_____)___________________.
Social Services can give you education and counseling about birth control and can assist you in getting medical care to help you plan for your desired family or to prevent unwanted pregnancies.
Even if your application for Public Assistance or Medical Assistance was denied, Social Services may provide information and education about family planning for up to 90 days from the date you applied.
For further information, please contact your services worker or call the general phone number on the front of this notice.
If you know of children under the age of 19 who do not have health care coverage, call
Regulations require that you immediately notify this Department of any changes in needs, income, resources, living arrangements or address.
Although you may no longer be able to get Public Assistance, SNAP Benefits or Medical Assistance, you still may be able to get help with your heating costs by applying for the Home Energy Assistance Program (HEAP). You can get more information on HEAP by calling the general telephone number on the front page of this notice.
SEE THE BACK OF PART B
FOR YOUR CONFERENCE AND FAIR HEARING RIGHTS.