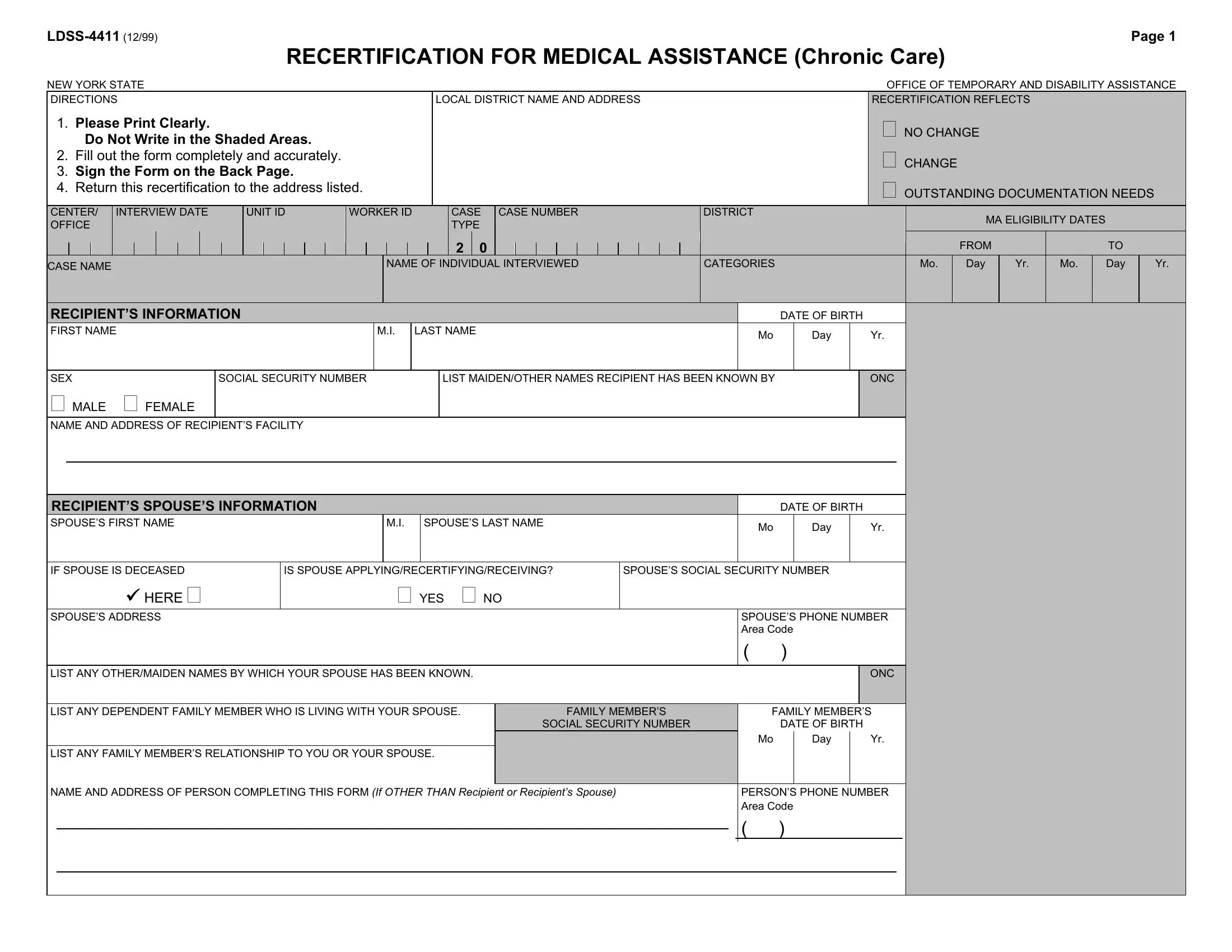
The LDSS-4411 form is an essential document for individuals in New York state seeking to recertify for Medical Assistance, particularly for chronic care. Outlined by the New York State Office of Temporary and Disability Assistance, this form serves as a comprehensive resource for capturing an applicant's vital information, changes in circumstances, and financial data crucial for determining continued eligibility for medical aid. Applicants are instructed to fill out the form with clear and accurate data, covering personal details, spouse information, and any dependent living with the spouse. It involves detailing resources, expected incomes, health insurance statuses, and even housing expenses, ensuring a holistic overview of the applicant's financial and living conditions. The form also asks for a thorough declaration of any transferred assets, aiming to prevent fraud and ensure that assistance goes to those genuinely in need. Moreover, the LDSS-4411 includes vital consents and agreements concerning Medicare, Direct Payment, and potential penalties for falsification of information or failure to disclose essential data. It underscores the importance of honesty and full disclosure in the process of applying for or recertifying for medical assistance, highlighting the legal and ethical responsibilities bestowed upon the applicant and their family members.
| Question | Answer |
|---|---|
| Form Name | Ldss 4411 Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | recertification assistance form online, recertification assistance form, ldss 4411 form online, ldss 3559 form |