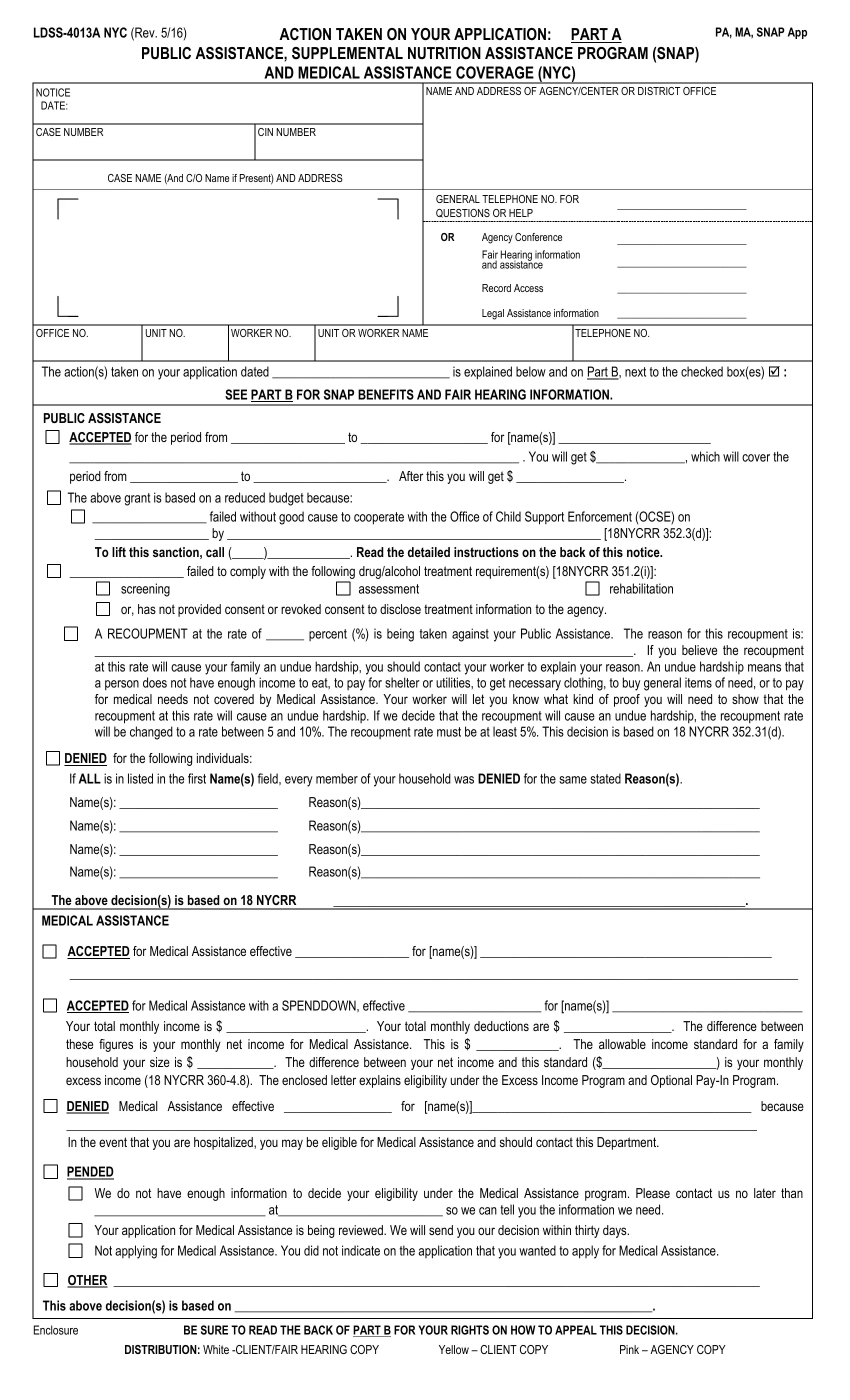
In navigating the complexities of acquiring public assistance, healthcare, and nutritional support, individuals and families often find themselves faced with paperwork that is both crucial and complex. One such document is the LDSS-4013A form, a vital communication from New York City's social services departments regarding the actions taken on applications for Public Assistance, the Supplemental Nutrition Assistance Program (SNAP), and Medical Assistance. Updated in May 2016, this form serves multiple functions. It notifies applicants about the decisions made on their applications—whether accepted, denied, pended, or other actions—and provides the specifics of any public assistance granted, including financial amounts and coverage periods. Crucially, the form details reasons for any denials and directions for appealing decisions, which could range from non-cooperation with child support enforcement to failure to comply with drug and alcohol treatment requirements. The LDSS-4013A form also addresses recoupment rates, indicating the financial adjustments made to assistance payments and offering guidance on how to argue undue hardship. Furthermore, it serves as a doorway to additional resources and rights, including information on family planning services, Child Health Plus coverage for those under 19, and contact details for further assistance. With sections dedicated to notifying applicants of their rights to appeal decisions, request agency conferences, access legal assistance, and more, the LDSS-4013A form epitomizes the intersection of administrative process and the individual's pursuit of assistance, embodying a critical step in navigating the often challenging path to obtaining essential support.
| Question | Answer |
|---|---|
| Form Name | Ldss 4013A Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | w 532 form, form 532, w 532 letter to past or present employer, form w 532 |