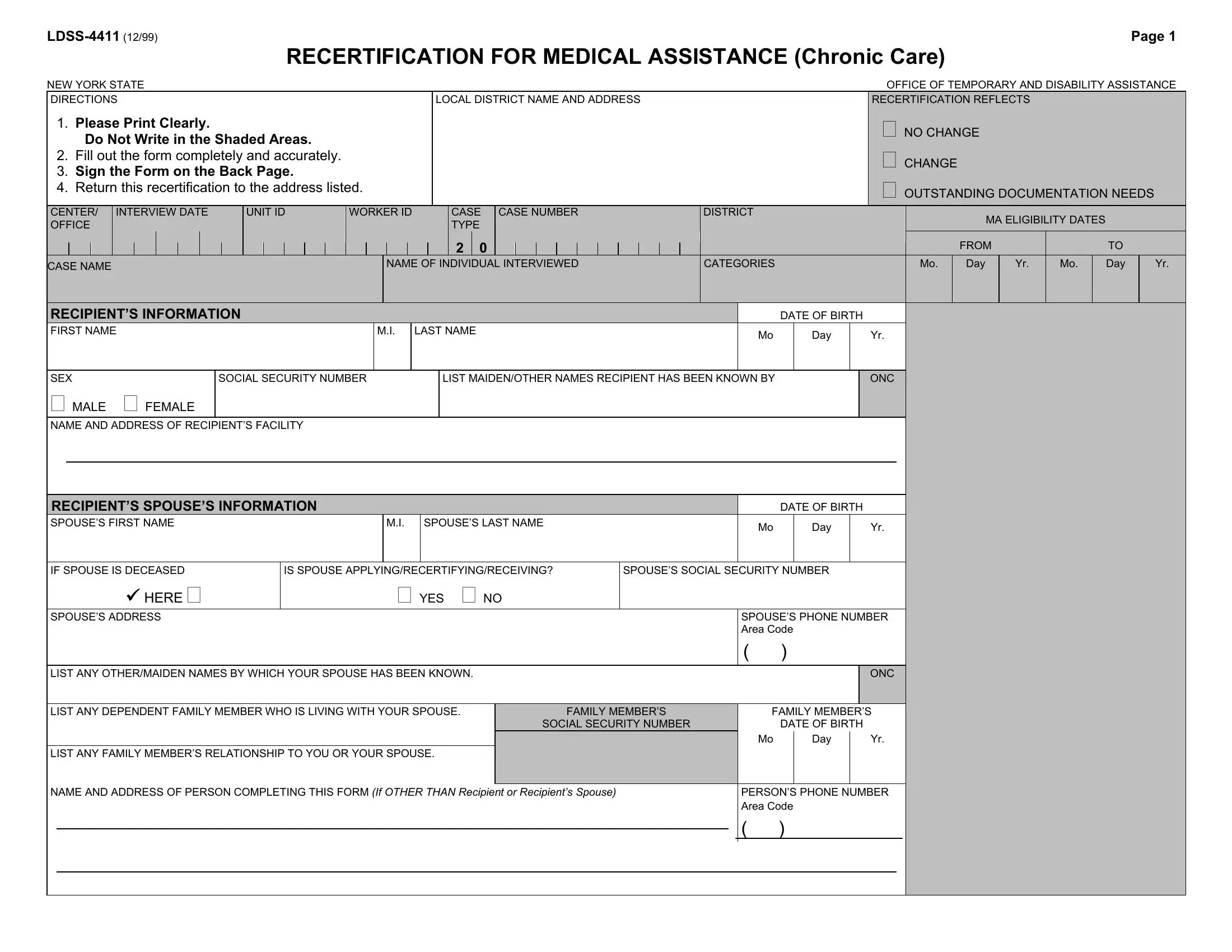
The LDSS-4411 form is an essential document for individuals in New York state seeking to recertify for Medical Assistance, particularly for chronic care. Outlined by the New York State Office of Temporary and Disability Assistance, this form serves as a comprehensive resource for capturing an applicant's vital information, changes in circumstances, and financial data crucial for determining continued eligibility for medical aid. Applicants are instructed to fill out the form with clear and accurate data, covering personal details, spouse information, and any dependent living with the spouse. It involves detailing resources, expected incomes, health insurance statuses, and even housing expenses, ensuring a holistic overview of the applicant's financial and living conditions. The form also asks for a thorough declaration of any transferred assets, aiming to prevent fraud and ensure that assistance goes to those genuinely in need. Moreover, the LDSS-4411 includes vital consents and agreements concerning Medicare, Direct Payment, and potential penalties for falsification of information or failure to disclose essential data. It underscores the importance of honesty and full disclosure in the process of applying for or recertifying for medical assistance, highlighting the legal and ethical responsibilities bestowed upon the applicant and their family members.
| Question | Answer |
|---|---|
| Form Name | Ldss 4411 Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | recertification assistance form online, recertification assistance form, ldss 4411 form online, ldss 3559 form |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Page 1 |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
RECERTIFICATION FOR MEDICAL ASSISTANCE (Chronic Care) |
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
NEW YORK STATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OFFICE OF TEMPORARY AND DISABILITY ASSISTANCE |
|||||||||||||||||||
DIRECTIONS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LOCAL DISTRICT NAME AND ADDRESS |
|
|
|
|
|
|
RECERTIFICATION REFLECTS |
|
|
|
|
|
|||||||||||||||||||||||||||
1. Please Print Clearly. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NO CHANGE |
|
|
|
|
|
|
|
||||||||||||
|
Do Not Write in the Shaded Areas. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CHANGE |
|
|
|
|
|
|
|
|
||||||||||||||||||
2. Fill out the form completely and accurately. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
3. Sign the Form on the Back Page. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OUTSTANDING DOCUMENTATION NEEDS |
|||||||||||||||||||||||||||
4. Return this recertification to the address listed. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
CENTER/ |
INTERVIEW DATE |
|
|
UNIT ID |
WORKER ID |
|
|
|
|
|
CASE |
CASE NUMBER |
DISTRICT |
|
|
|
|
|
|
|
|
|
|
MA ELIGIBILITY DATES |
|
|
|
|||||||||||||||||||||||||||||
OFFICE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TYPE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
0 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FROM |
|
|
TO |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
CASE NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAME OF INDIVIDUAL INTERVIEWED |
CATEGORIES |
|
|
|
|
|
|
|
Mo. |
|
Day |
|
Yr. |
Mo. |
|
Day |
|
Yr. |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
RECIPIENT’S INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE OF BIRTH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
FIRST NAME |
|
|
|
|
|
|
|
|
|
M.I. |
|
LAST NAME |
|
|
|
|
|
|
|
|
Mo |
|
Day |
|
|
Yr. |
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
SEX |
|
|
|
|
|
SOCIAL SECURITY NUMBER |
|
|
|
|
LIST MAIDEN/OTHER NAMES RECIPIENT HAS BEEN KNOWN BY |
|
|
|
|
ONC |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
MALE |
FEMALE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
NAME AND ADDRESS OF RECIPIENT’S FACILITY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
RECIPIENT’S SPOUSE’S INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE OF BIRTH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
SPOUSE’S FIRST NAME |
|
|
|
|
|
|
|
|
|
|
M.I. |
|
SPOUSE’S LAST NAME |
|
|
|
|
|
|
|
|
Mo |
|
Day |
|
|
Yr. |
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
IF SPOUSE IS DECEASED |
|
|
|
|
IS SPOUSE APPLYING/RECERTIFYING/RECEIVING? |
|
|
|
SPOUSE’S SOCIAL SECURITY NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
|
Y HERE |
|
|
|
|
|
|
|
|
|
|
YES NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
SPOUSE’S ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SPOUSE’S PHONE NUMBER |
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Area Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
LIST ANY OTHER/MAIDEN NAMES BY WHICH YOUR SPOUSE HAS BEEN KNOWN. |
|
|
|
|
|
|
|
|
|
|
|
|
|
ONC |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||
LIST ANY DEPENDENT FAMILY MEMBER WHO IS LIVING WITH YOUR SPOUSE. |
|
FAMILY MEMBER’S |
|
FAMILY MEMBER’S |
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SOCIAL SECURITY NUMBER |
|
|
DATE OF BIRTH |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mo |
|
Day |
|
Yr. |
|
|
|
|
|
|
|
|
|||||
LIST ANY FAMILY MEMBER’S RELATIONSHIP TO YOU OR YOUR SPOUSE. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||
NAME AND ADDRESS OF PERSON COMPLETING THIS FORM (If OTHER THAN Recipient or Recipient’s Spouse) |
|
PERSON’S PHONE NUMBER |
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Area Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
( )
|
|
|
|
|
|
|
|
|
|
Page 2 |
|||
RESOURCES |
|
|
|
|
|
|
|
|
|
|
DO NOT WRITE IN SHADED AREA |
||
LIST ANY RESOURCES THAT THE RECIPIENT MAY HAVE: |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|||||||
|
|
|
|
YES |
NO |
|
$ |
VALUE |
|
|
ACCOUNT NUMBER |
LOCATION |
|
Personal Incidental Account (PIA) |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Savings Account (Checking/Savings/ |
|
|
|
|
|
|
|
|
|
|
|||
Certificate of Deposit in Bank, |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|||
Credit Union) |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Expect Lawsuit Settlement, Inheritance |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Trust Fund |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Life Insurance |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Annuity |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Stocks, Bonds, Savings Bonds |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Real Estate (Including Vacation Property |
|
|
|
|
|
|
|
|
|
|
|||
and Homestead) |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Own Home |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mutual Fund |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IRA, KEOGH, |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other Pension or Retirement Account |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Burial Fund, Burial Trust, Burial Space |
|
|
|
|
|
|
|
|
|
|
|||
(Cemetery Plot), Funeral Agreement |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other Resources (Please Specify) |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Motor Vehicle |
|
|
|
Value |
|
|
Year |
Make |
Model |
|
|||
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
HAVE YOU OR YOUR SPOUSE SOLD, GIVEN AWAY, OR TRANSFERRED ANY CASH, INCOME, REAL ESTATE, OR OTHER ASSET |
|
||||||||||||
WITHIN THE PAST 36 MONTHS (60 MONTHS FOR TRUSTS)? |
|
|
|
||||||||||
YES |
NO |
|
ASSET |
|
VALUE |
|
|
WHO DID IT GO TO? |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|