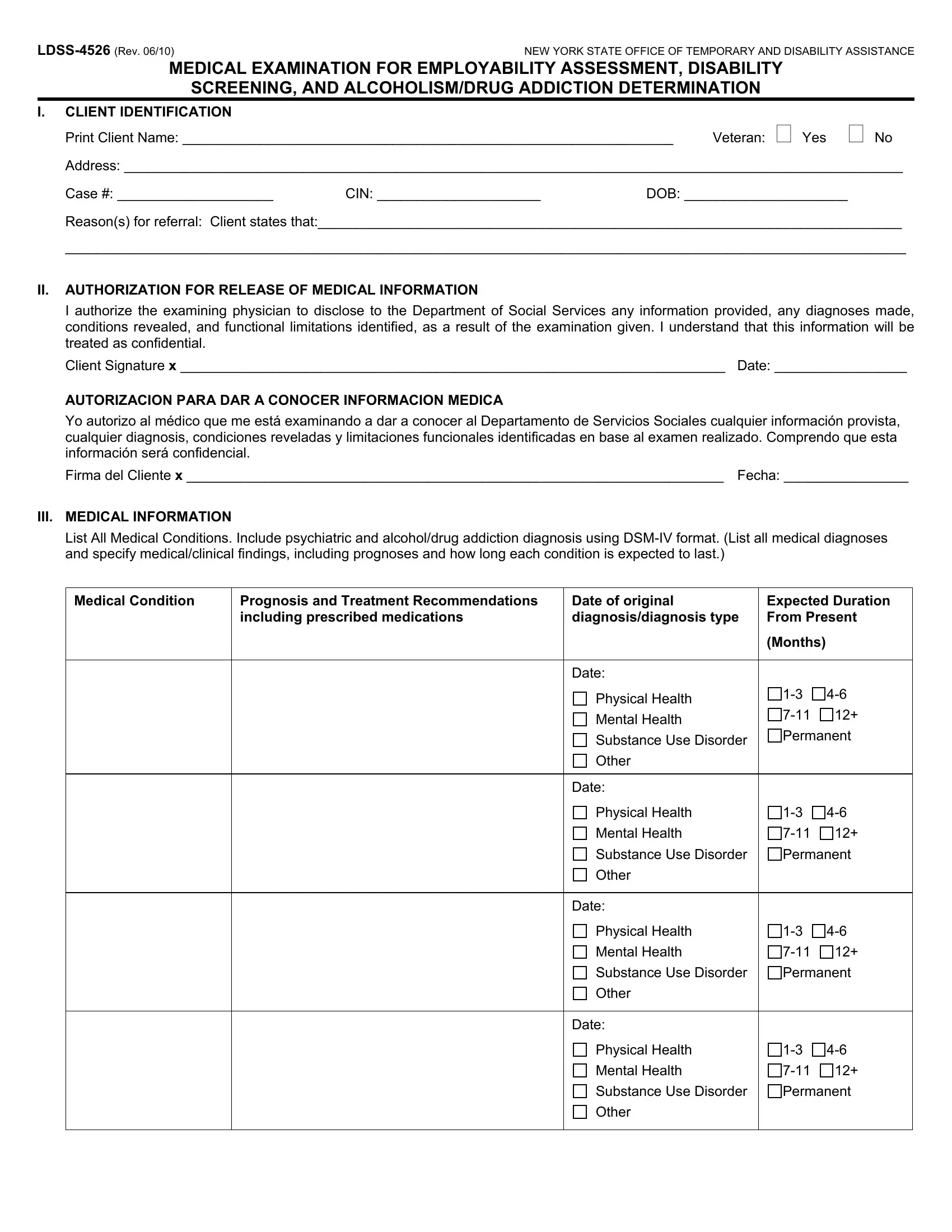
The LDSS-4526 form, a product of the New York State Office of Temporary and Disability Assistance, serves a critical function in bridging health assessments with social service needs. By drawing a comprehensive picture that encompasses medical examinations for employability assessment, disability screening, and determinations related to alcoholism and drug addiction, this document encapsulates a multi-layered approach to social service qualification and provision. Within its sections, the form meticulously captures client identification details, necessitates an authorization for the release of medical information, and anchors an in-depth medical catalog encompassing both physical and psychological health realms, in addition to substance use disorders. Furthermore, it assesses functional limitations directly correlated with medical findings, sketches treatment history, identifies current treatment programs, and outlines work activity limitations, paving the way for a nuanced understanding of the client’s health and social service eligibility and needs. Notably, its design also allows for the screening of potential referrals to Supplemental Security Income (SSI), underscoring its role as a critical tool in social service and healthcare provider arsenals.
| Question | Answer |
|---|---|
| Form Name | Ldss 4526 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | ldss 4526 disability, new york ldss 4526 form, ldss 4526 determination, medical examination assessment |