Are you having trouble completing the required LDSS 4992 form? This document is used by the New York Office of Temporary and Disability Assistance to verify an individual’s status for nutrition programs such as SNAP, cash assistance, Medicaid and TANF. Completing this form can be a frustrating task if you are not familiar with the requirements or have never filled out one before. In this blog post we will provide information about what this form is, why it's important, who needs to complete it and how you can fill it out correctly to save time and hassle. Keep reading if you're looking for some helpful guidance in navigating through the process!
| Question | Answer |
|---|---|
| Form Name | Ldss 4992 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | weatherization, ineligible, misrepresentation, ldss 4992 revised 5 17 |
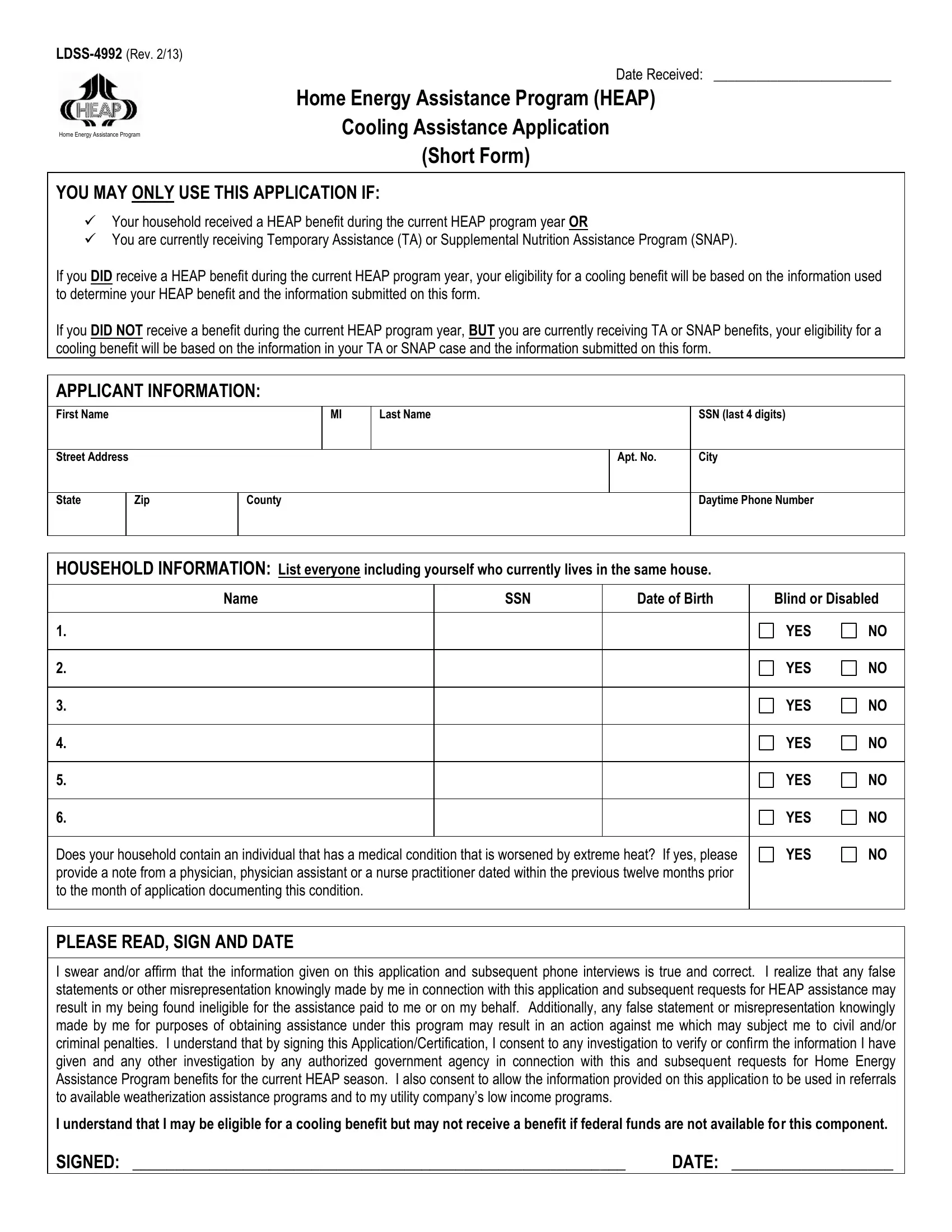
Date Received: _________________________
Home Energy Assistance Program (HEAP)
Home Energy Assistance Program
Cooling Assistance Application
(Short Form)
YOU MAY ONLY USE THIS APPLICATION IF:
Your household received a HEAP benefit during the current HEAP program year OR
You are currently receiving Temporary Assistance (TA) or Supplemental Nutrition Assistance Program (SNAP).
If you DID receive a HEAP benefit during the current HEAP program year, your eligibility for a cooling benefit will be based on the information used to determine your HEAP benefit and the information submitted on this form.
If you DID NOT receive a benefit during the current HEAP program year, BUT you are currently receiving TA or SNAP benefits, your eligibility for a cooling benefit will be based on the information in your TA or SNAP case and the information submitted on this form.
APPLICANT INFORMATION:
First Name
MI
Last Name
SSN (last 4 digits)
Street Address
Apt. No.
City
State
Zip
County
Daytime Phone Number
HOUSEHOLD INFORMATION: List everyone including yourself who currently lives in the same house.
Name |
SSN |
Date of Birth |
Blind or Disabled |
|
|
|
|
|
|
1. |
|
|
YES |
NO |
|
|
|
|
|
2. |
|
|
YES |
NO |
|
|
|
|
|
3. |
|
|
YES |
NO |
|
|
|
|
|
4. |
|
|
YES |
NO |
|
|
|
|
|
5. |
|
|
YES |
NO |
|
|
|
|
|
6. |
|
|
YES |
NO |
|
|
|
|
|
Does your household contain an individual that has a medical condition that is worsened by extreme heat? If yes, please |
YES |
NO |
||
provide a note from a physician, physician assistant or a nurse practitioner dated within the previous twelve months prior |
|
|
||
to the month of application documenting this condition. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PLEASE READ, SIGN AND DATE
I swear and/or affirm that the information given on this application and subsequent phone interviews is true and correct. I realize that any false statements or other misrepresentation knowingly made by me in connection with this application and subsequent requests for HEAP assistance may result in my being found ineligible for the assistance paid to me or on my behalf. Additionally, any false statement or misrepresentation knowingly made by me for purposes of obtaining assistance under this program may result in an action against me which may subject me to civil and/or criminal penalties. I understand that by signing this Application/Certification, I consent to any investigation to verify or confirm the information I have given and any other investigation by any authorized government agency in connection with this and subsequent requests for Home Energy
Assistance Program benefits for the current HEAP season. I also consent to allow the information provided on this application to be used in referrals to available weatherization assistance programs and to my utility company’s low income programs.
I understand that I may be eligible for a cooling benefit but may not receive a benefit if federal funds are not available for this component.
SIGNED: __________________________________________________________ |
DATE: ___________________ |
|
FOR AGENCY USE ONLY |
|
|
Received a current HEAP Program year benefit: |
Regular |
Emergency |
|
|
Eligible |
Pended Start: ______________ |
End: ______________ |
|
Ineligible because: |
No Vulnerable Household Member |
|
|
|
Failed to Provide Information |
|
|
|
Over Income Limit (Code 5) |
|
|
|
Other |
|
Comments: |
|
Eligibility Determination Date: ____________ |
|
Worker Signature: _________________________________ Date: ____________ |
Supervisors Initials: _______ Date: ________ |