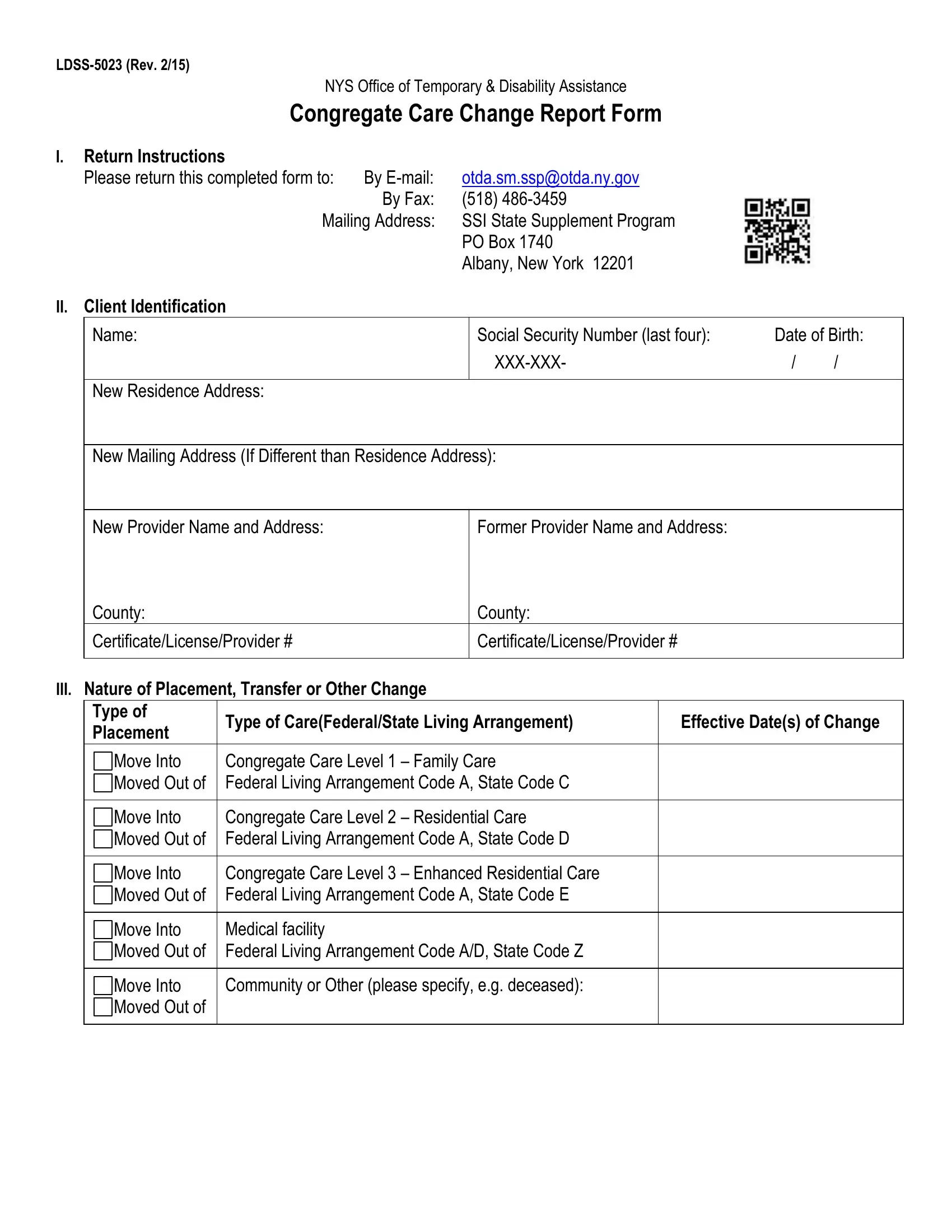
The LDSS-5023 form, issued by the New York State Office of Temporary & Disability Assistance, serves a crucial role in the administration of congregate care changes for individuals receiving assistance. This detailed document guides users through the process of reporting any shifts in living arrangements, whether it's moving into or out of various levels of congregate care, medical facilities, or other specified living situations. It meticulously collects client identification information, including name, social security number, and address changes. Additionally, it covers a broad range of reportable changes, from the nature of placement or transfer to adjustments in custody for minors, income fluctuations, and resource tallies. The form also facilitates the authorization for direct deposits of State Supplement Program (SSP) benefits, requiring detailed banking information and signatures from the payee or the resident themselves, depending on the context. With return instructions clear on submission via email, fax, or mail, and contact information for further assistance, the LDSS-5023 form embodies a comprehensive approach to ensuring that individuals in congregate care settings have their changes accurately reported and processed, reflecting the state’s commitment to the welfare of its residents.
| Question | Answer |
|---|---|
| Form Name | Ldss 5023 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | form, ny, social, representative |