
If you want to fill out 401 statement, you won't need to install any kind of software - just try using our PDF editor. To retain our tool on the cutting edge of convenience, we strive to implement user-oriented capabilities and enhancements on a regular basis. We are always grateful for any feedback - join us in remolding the way you work with PDF files. Here's what you'd want to do to start:
Step 1: First, access the tool by pressing the "Get Form Button" at the top of this page.
Step 2: The editor will let you change the majority of PDF files in many different ways. Improve it by including personalized text, correct existing content, and put in a signature - all at your fingertips!
This PDF form will need some specific information; in order to ensure correctness, please make sure to take into account the suggestions directly below:
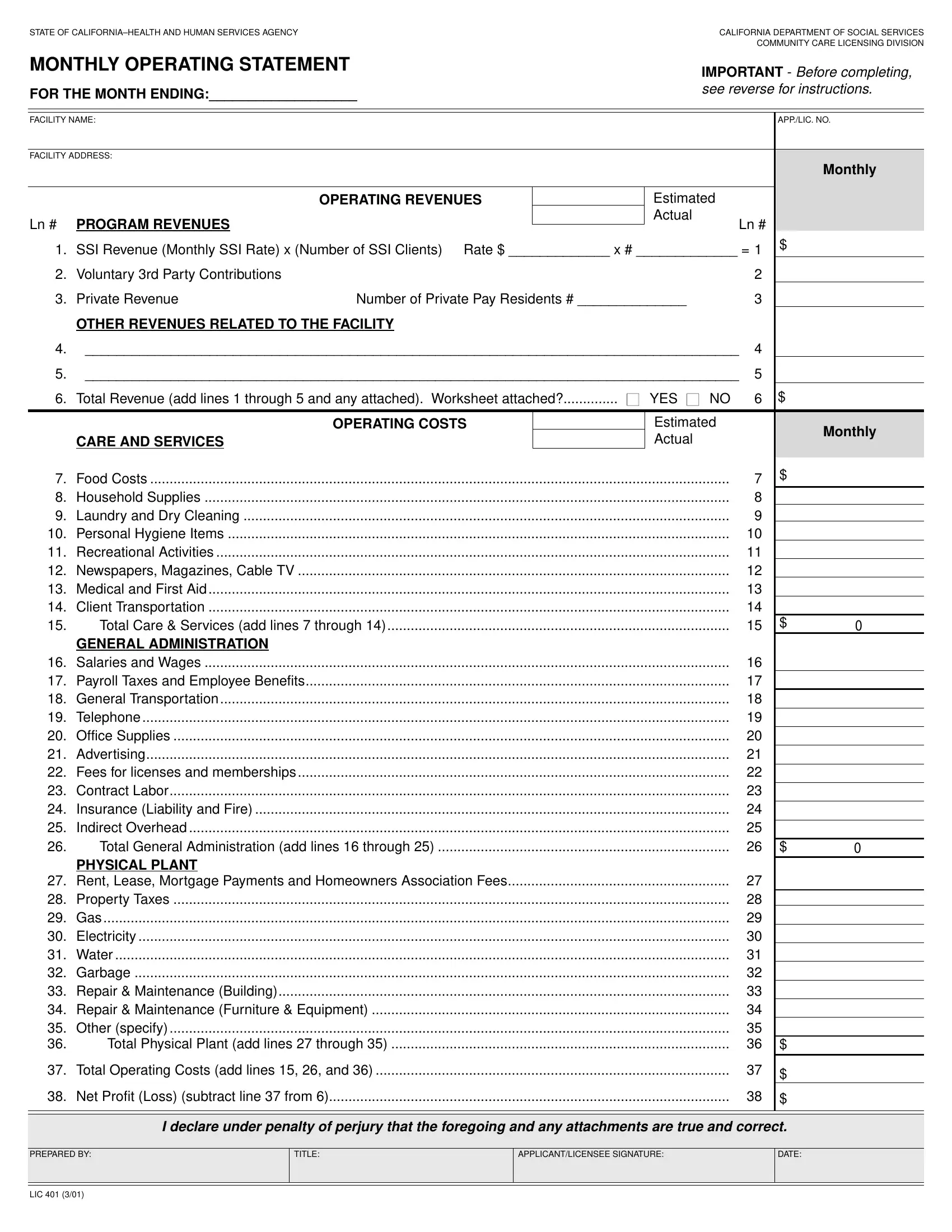
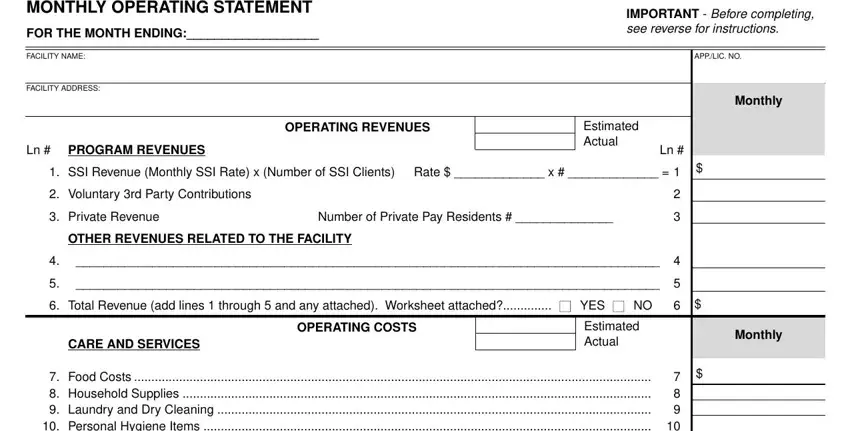
1. The 401 statement will require specific details to be inserted. Be sure the following fields are completed:
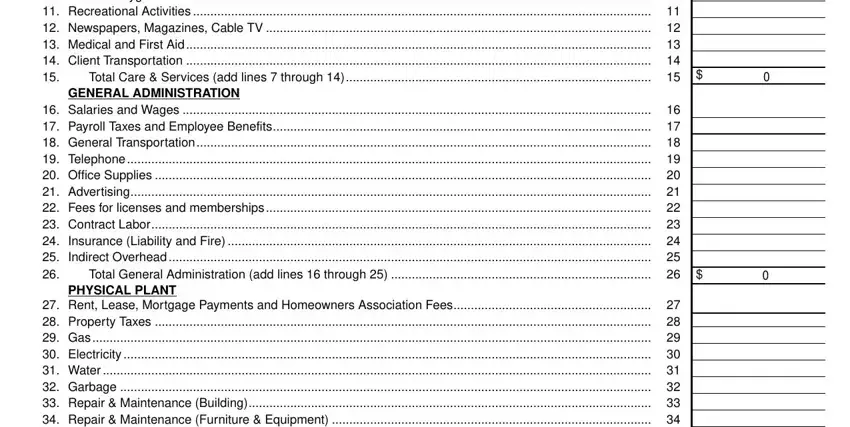
2. Given that the last array of fields is completed, it's time to insert the essential details in Food Costs Household Supplies, GENERAL ADMINISTRATION, Salaries and Wages Payroll, PHYSICAL PLANT, and Rent Lease Mortgage Payments and in order to proceed further.
3. The following segment is typically pretty easy, Rent Lease Mortgage Payments and, Total Operating Costs add lines, Net Profit Loss subtract line, I declare under penalty of perjury, PREPARED BY, TITLE, APPLICANTLICENSEE SIGNATURE, DATE, and LIC - all these fields needs to be filled in here.
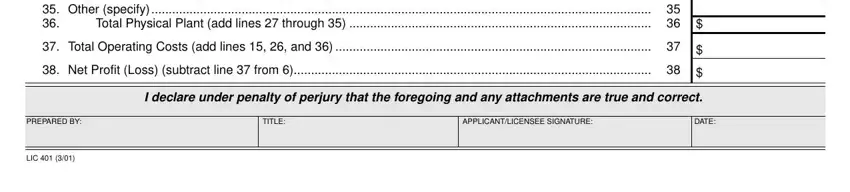
When it comes to DATE and Total Operating Costs add lines, be sure you don't make any mistakes in this current part. These are certainly the most important ones in this document.
Step 3: Immediately after going through the entries, click "Done" and you are all set! Join us today and easily get access to 401 statement, available for download. Each change made is handily saved , meaning you can change the form later when required. FormsPal is devoted to the personal privacy of our users; we make sure all information processed by our tool continues to be secure.