Completing the LIC 624 Form with attention to detail and accuracy is essential for effectively managing incident reports in community care settings.
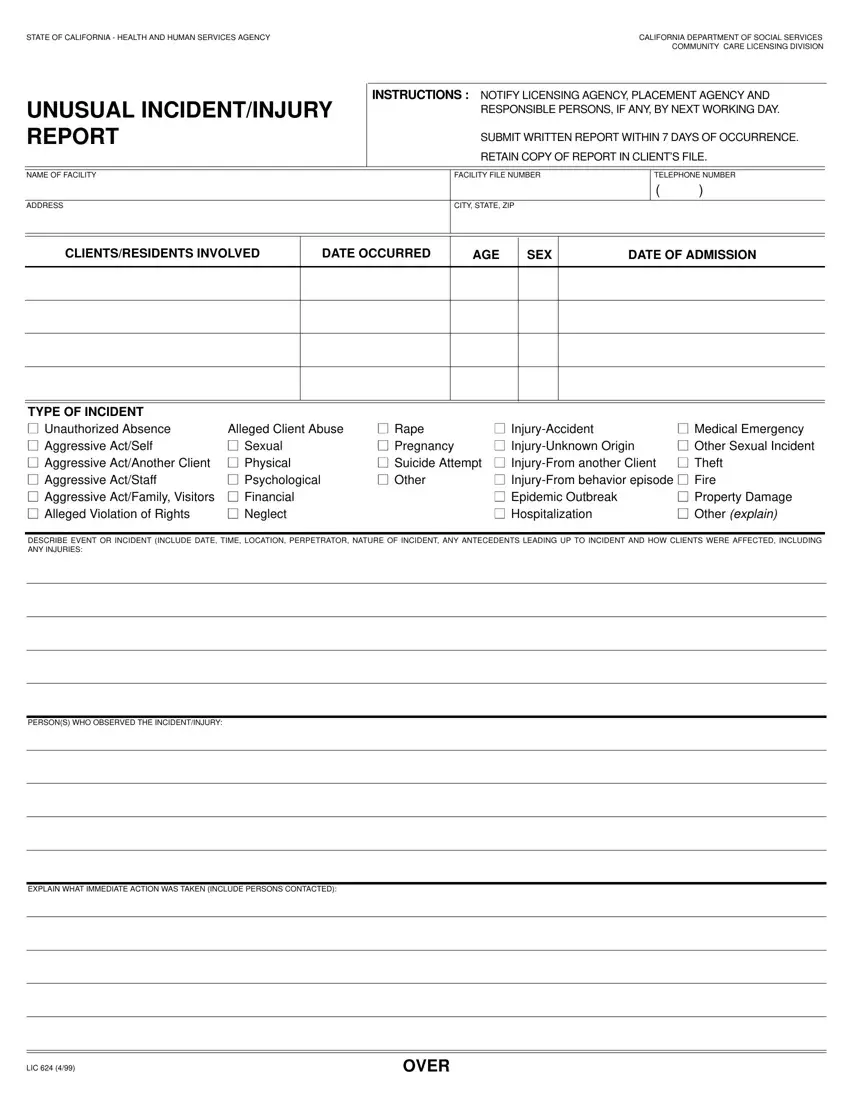
1. Facility and Incident Details
Print the facility's name, facility file number, and the location's city, state, and zip code in the designated areas at the top of the form.
2. Describe the Event or Incident
Provide a detailed description of the event or incident, including the date, time, and location. Mention any known perpetrators, describe the nature of the incident, and list any antecedents leading up to the incident. It's important to describe how the clients were affected, including any injuries sustained.
3. Observations and Immediate Actions Taken
Record the names of persons who observed the incident. Explain the immediate actions taken in response to the incident, including the names of persons contacted. It might involve first aid measures, calling emergency services, or notifying guardians and family members.
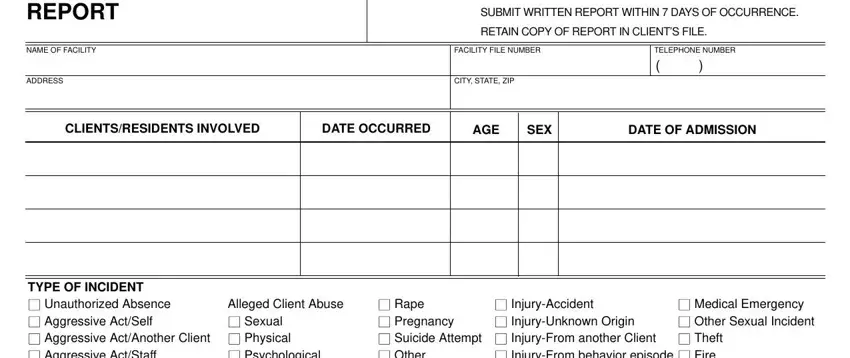
4. Client and Incident Type Information
Fill in the sections concerning the clients/residents involved, including the date the incident occurred, their ages, genders, and dates of admission. Check the appropriate boxes to indicate the type of incident, such as unauthorized absence, alleged abuse, medical emergency, etc.
5. Document Medical Treatment
If medical treatment was necessary, check "Yes" and provide details about the nature of the treatment, the attending physician's name, and where the treatment was administered.
6. Report Submission and Review
Complete the sections for who submitted the report and who reviewed/approved it. Include names, titles, and the date the report was submitted and reviewed.
7. Notify Relevant Agencies and Persons
List all agencies and individuals who were notified about the incident. Specify names and telephone numbers for each, such as licensing bodies, protective services, law enforcement, and placement agencies.
8. Detail Follow-Up Actions
If any follow-up treatment or further actions are anticipated, describe them here. Include information on who will be responsible for these actions and the expected outcomes.
9. Additional Comments
Provide any additional comments or observations in the final section of the form. This might cover insights into how the incident could have been prevented or how procedures might be improved.
