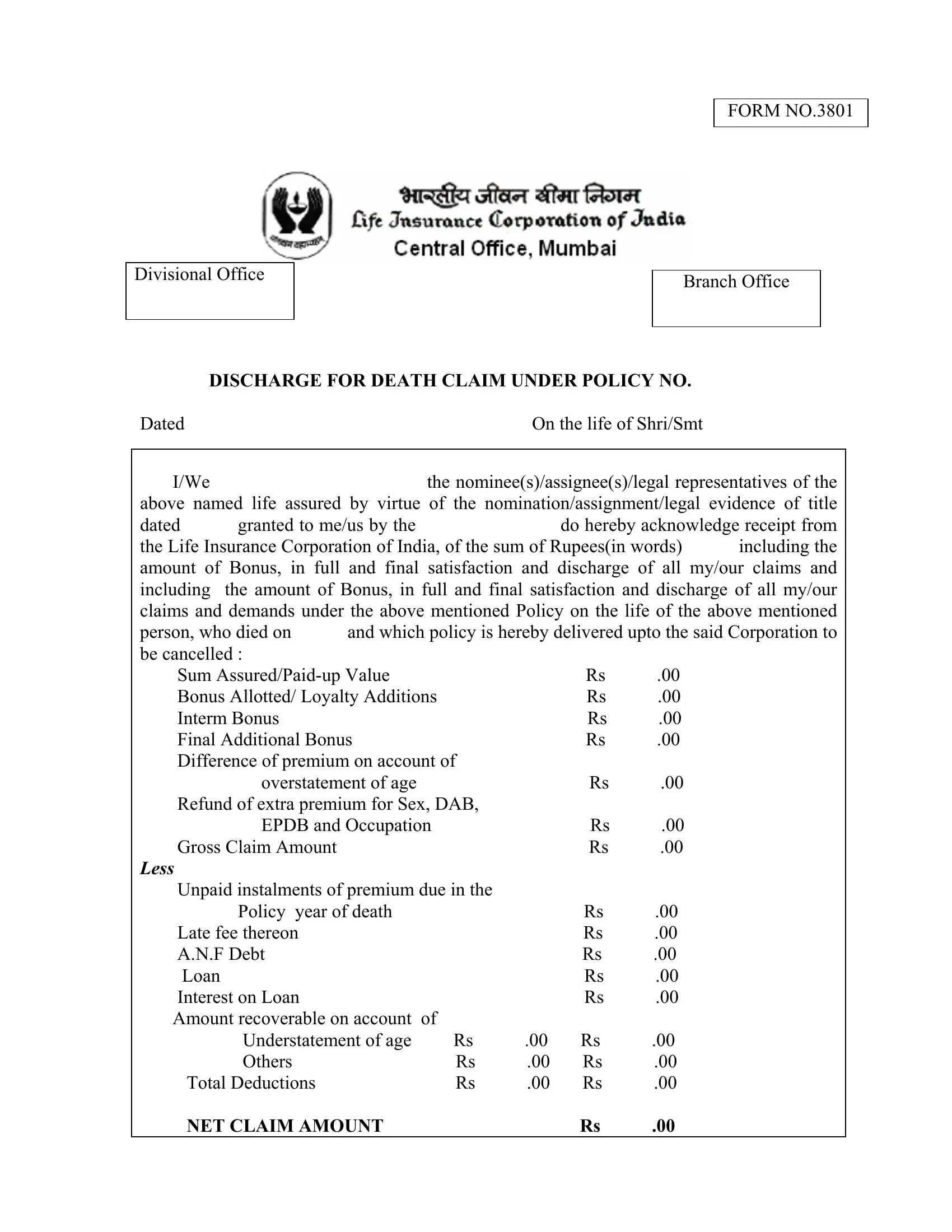
When someone passes away, dealing with life insurance can be one of the biggest tasks for the family or beneficiaries left behind. The LIC Death Claim Form No. 3801 serves as a crucial document during such poignant times. This form is used by nominees, assignees, or legal representatives to formally request and acknowledge the receipt of claim funds from a deceased's life insurance policy under the Life Insurance Corporation of India. It provides detailed fields for summarizing the policy under which the death claim is made, including specifics like the sum assured, bonuses, any applicable loans, and the net claim amount after deductions. Alongside financial details, the form gives clear instructions on how it should be completed, specifying the presence needed of an advocate, various officials, or officers during the signing. Furthermore, the inclusion of personal identifiers, such as father's and husband's names for female claimants and requirements regarding the attestation of thumb impressions, underlines the form's emphasis on precise verification and authentication. This approach not only secures the transaction for all parties involved but also outlines a clear procedural path for disbursing the death claim, ensuring that the process is as straightforward and respectful as possible during a difficult time.
| Question | Answer |
|---|---|
| Form Name | LIC Death Claim Form 3801 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | lic form 3801, lic form 3801 in hindi pdf, lic claim form, form 3801 lic |
Divisional Office
FORM NO.3801
Branch Office
DISCHARGE FOR DEATH CLAIM UNDER POLICY NO.
Dated |
On the life of Shri/Smt |
|
|
I/We |
the nominee(s)/assignee(s)/legal representatives of the |
above named life assured by virtue of the nomination/assignment/legal evidence of title
dated |
granted to me/us by the |
do hereby acknowledge receipt from |
|
the Life Insurance Corporation of India, of the sum of Rupees(in words) |
including the |
||
amount of Bonus, in full and final satisfaction and discharge of all my/our claims and including the amount of Bonus, in full and final satisfaction and discharge of all my/our claims and demands under the above mentioned Policy on the life of the above mentioned
person, who died on |
and which policy is hereby delivered upto the said Corporation to |
||||
be cancelled : |
|
|
|
|
|
Sum |
|
|
Rs |
.00 |
|
Bonus Allotted/ Loyalty Additions |
|
|
Rs |
.00 |
|
Interm Bonus |
|
|
|
Rs |
.00 |
Final Additional Bonus |
|
|
Rs |
.00 |
|
Difference of premium on account of |
|
|
|
||
overstatement of age |
|
|
Rs |
.00 |
|
Refund of extra premium for Sex, DAB, |
|
|
|
||
EPDB and Occupation |
|
|
Rs |
.00 |
|
Gross Claim Amount |
|
|
Rs |
.00 |
|
LESS |
|
|
|
|
|
Unpaid instalments of premium due in the |
|
|
|
||
Policy |
year of death |
|
|
Rs |
.00 |
Late fee thereon |
|
|
Rs |
.00 |
|
A.N.F Debt |
|
|
|
Rs |
.00 |
Loan |
|
|
|
Rs |
.00 |
Interest on Loan |
|
|
Rs |
.00 |
|
Amount recoverable on account of |
|
|
|
|
|
Understatement of age |
Rs |
.00 |
Rs |
.00 |
|
Others |
|
Rs |
.00 |
Rs |
.00 |
Total Deductions |
Rs |
.00 |
Rs |
.00 |
|
NET CLAIM AMOUNT |
|
|
Rs |
.00 |
|
Dated at |
this |
day of |
|
||
Signed by Shri/Smt |
|
|
|
|
|
|
1 Re. |
|
|
||
in the presence of |
* |
|
|
|
|
|
Revenue |
|
|
||
|
|
|
|
|
|
Signature of witness |
|
Stamp |
|
|
|
|
|
|
|
||
Full Name |
|
Signature of claimant/s |
|||
Designation |
|
|
|
|
|
Address |
|
|
|
|
|
|
|
Fathers Name |
: |
||
|
|
Husband Name : |
|||
|
|
Address |
: |
||
Notes :
(1)Payment will be made by a crossed and order cheque, if payment is desired by M.O (Net upto Rs. 1000/- only ) or a Demand Draft, it can be made at the claimant’s cost and at his/her risk and responsibility on his/her signing the following note of request.
I/We hereby request the Corporation to pay the aforesaid amount by M.O
/Demand Draft on theBank,at my/our own risk and responsibility. I/We further agree to the M.O. Commission/Bank Charges being deducted from the claim amount .
(Signature of Claimant/s)
(2)This form must be completed before (1) an advocate, (2) an Agent of the Corporation (who is a member of an Agents club at the level of Divisional Manager’s club or above), (3) a Bank Manager, (4) a Block Development Officer, (5) a Commissioner of Oaths, (6) a Doctor, (7) a Gazetted Officer, (8) a Head Master of a High School, (9) a Head Post Master or Departmental
(3)If more than one person have signed the Discharge Form, the names of all the persons should be stated.
(4)A female when signing, must add her father’s as well as her husband’s name after her
own, describing herself as a daughter of Shri |
and wife/widow of shri |
(5)“In case the claimant affixes thumb impression or if this form is signed by more than one person and payment is desired to be made to only one of them as per the following Note of Authority completed and by all of them, the thumb impression or the signatures on the letter of authority must be attested by an Agent of the Corporation
(who is a member of the club at the level of Divisional Manager’s club and above), a Block Development Officer, a Magistrate, or an Officer or Development Officer (with at least 3 years’ service as Development Officer) of LIC or a Bank Manager of Branch of State Bank of India or of one of the nationalized banks (provided the attesting Branch Manager signs after affixing an official rubber stamp giving his name and designation as also the name and address of the Bank where he is working) or the Principal/Head Master of a local High School or Higher Secondary School run by Government. Where thumb marks are affixed, the attesting official must make the following signature under his signature :
“Shri/Smt |
son/daughter of Shri |
and wife/widow of Shri |
has affixed |
||
his/her thumb marks in my presence after understanding the contents thereof.” |
|||||
|
|
|
|
|
|
Place |
|
|
|
Date |
|
We hereby authorize and request the Life Insurance Corporation of India to pay the |
|||||
within mentioned amount of Rs. |
.00 to Shri/Smt |
. |
|
||
Signed by the parties within mentioned in the |
|
(1) |
|
||
presence of :- |
|
|
|
|
|
|
|
|
|
(2) |
|
Witness |
|
|
|
|
|
Signature |
|
|
|
(3) |
|
(Signature in Full)
Full Name :
Designation :
Address :
|
I certify that the contents of this Note of Authority were explained by me to |
Shri/Smt |
and he/she/they have agreed to payment being made to |
Shri/Smt |
the authorised party. |
|
(Signature of Witness) |