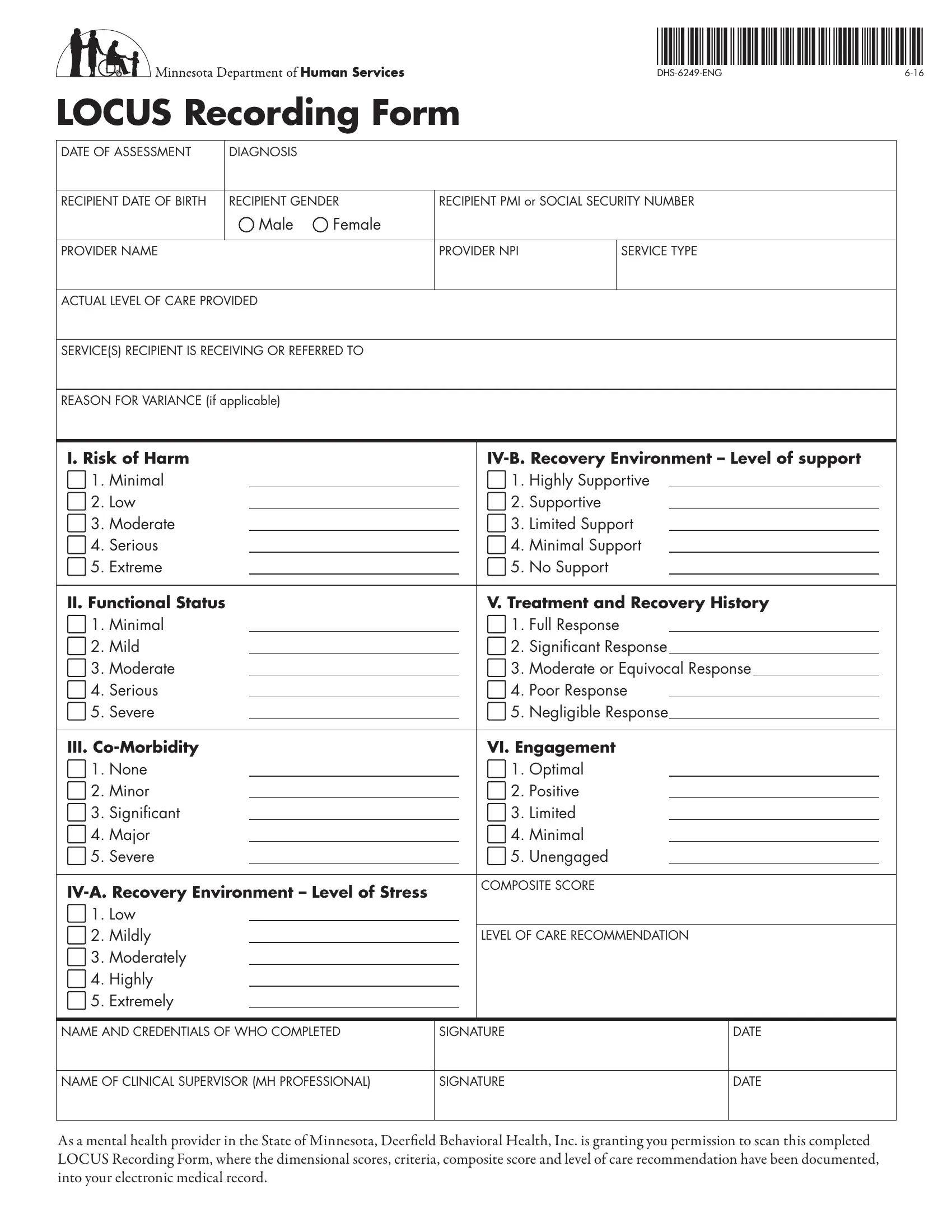
The Locus Worksheet form, identified as DHS-6249-ENG, serves as a critical tool in the mental health sector, particularly within the State of Minnesota. Designed to systematically evaluate the needs and appropriate level of care for individuals receiving mental health services, this comprehensive form guides providers through a structured assessment process, encompassing a wide array of factors crucial for determining the most suitable care pathway. It includes sections on the date of assessment, recipient's diagnosis, demographic details, and detailed provider information. Significantly, the form evaluates through a multi-dimensional approach, covering risk of harm, functional status, co-morbidity, recovery environment, treatment history, and engagement level, each rated with a defined scale to ensure consistent application. The outcome includes a composite score and a level of care recommendation, taking into account potential variances and the rationale for any discrepancy between recommended and actual care levels. This process not only standardizes care assessments across providers but also emphasizes the importance of tailored healthcare plans that align with the unique needs of each recipient. Furthermore, the inclusion of signature spaces for the assessing professional and, if necessary, a clinical supervisor, underscores the accountability and professionalism expected in these assessments. By permitting the scanning of this document into electronic medical records, the form facilitates streamlined documentation and sharing of critical assessment outcomes, enhancing the continuum of care.
| Question | Answer |
|---|---|
| Form Name | Locus Worksheet Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | locus assessment form, locus worksheet pdf 2021, mn locus form, dhs 6249 eng |
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
||||||
LOCUS Recording Form |
||||||||||||||||
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
DATE OF ASSESSMENT |
|
DIAGNOSIS |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
||||||
RECIPIENT DATE OF BIRTH |
|
RECIPIENT GENDER |
RECIPIENT PMI or SOCIAL SECURITY NUMBER |
|
||||||||||||
|
|
|
|
|
Male |
Female |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
PROVIDER NAME |
|
|
|
PROVIDER NPI |
|
SERVICE TYPE |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
ACTUAL LEVEL OF CARE PROVIDED |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
||||||
SERVICE(S) RECIPIENT IS RECEIVING OR REFERRED TO |
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
REASON FOR VARIANCE (if applicable) |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
||||||
I. Risk of Harm |
|
|
|
|
|
|
||||||||||
1. |
Minimal |
|
|
|
|
|
1. |
Highly Supportive |
|
|
|
|||||
2. |
Low |
|
|
|
|
|
2. |
Supportive |
|
|
|
|||||
3. |
Moderate |
|
|
|
|
|
3. |
Limited Support |
|
|
|
|||||
4. |
Serious |
|
|
|
|
|
4. |
Minimal Support |
|
|
|
|||||
5. |
Extreme |
|
|
|
|
|
5. |
No Support |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
II. Functional Status |
|
|
|
|
|
V. Treatment and Recovery History |
|
|||||||||
1. |
Minimal |
|
|
|
|
|
1. |
Full Response |
|
|
|
|||||
2. |
Mild |
|
|
|
|
|
2. |
Significant Response |
|
|
|
|||||
3. |
Moderate |
|
|
|
|
|
3. |
Moderate or Equivocal Response |
|
|
|
|||||
4. |
Serious |
|
|
|
|
|
4. |
Poor Response |
|
|
|
|||||
5. |
Severe |
|
|
|
|
|
5. |
Negligible Response |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
III. |
|
|
|
|
|
VI. Engagement |
|
|||||||||
1. |
None |
|
|
|
|
|
1. |
Optimal |
|
|
|
|||||
2. |
Minor |
|
|
|
|
|
2. |
Positive |
|
|
|
|||||
3. |
Significant |
|
|
|
|
|
3. |
Limited |
|
|
|
|||||
4. |
Major |
|
|
|
|
|
4. |
Minimal |
|
|
|
|||||
5. |
Severe |
|
|
|
|
|
5. |
Unengaged |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMPOSITE SCORE |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
||||||||
1. |
Low |
|
|
|
|
|
|
|
|
|
|
|
|
|||
2. |
Mildly |
|
|
|
|
|
LEVEL OF CARE RECOMMENDATION |
|
||||||||
3. |
Moderately |
|
|
|
|
|
|
|
|
|
|
|
|
|||
4. |
Highly |
|
|
|
|
|
|
|
|
|
|
|
|
|||
5. |
Extremely |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAME AND CREDENTIALS OF WHO COMPLETED
SIGNATURE
DATE
NAME OF CLINICAL SUPERVISOR (MH PROFESSIONAL)
SIGNATURE
DATE
As a mental health provider in the State of Minnesota, Deerield Behavioral Health, Inc. is granting you permission to scan this completed LOCUS Recording Form, where the dimensional scores, criteria, composite score and level of care recommendation have been documented, into your electronic medical record.
Instructions for completing the
LOCUS Recording Form
Date of Assessment
he date the LOCUS assessment was completed.
Date of Birth
Month/Day/Year (MM/DD/YYYY)
Gender
Male or Female
Recipient PMI or Social Security number
PMI number is preferred over the social security number.
Diagnosis
Primary (Write in the full diagnostic name of the primary diagnosis or use the ICD code).
Provider Name, NPI and Service Type
NPI number and the name of the organization completing the LOCUS and what type of service is being provided by the staf completing the LOCUS assessment.
Actual Level of Care
What is the actual Level of Care the recipient is receiving? Write the actual name of the level (i.e. Medically Monitored
Service/Program Referred to
Write the current program(s) recipient is in or what program(s) recipient has been referred to (example: ARMHS, Day Treatment, Case Management, Psychiatry, housing programs, etc.). Please keep in mind that there may be multiple services used to reach an individual’s resource intensity needs.
Reason for Variance (if applicable)
If the service provided is at a diferent level of care from the level of care recommendation, provide the brief clinical justiication as to why the variance was made. Clinical justiication also needs to be documented in more detail as a separate document from the recording form.
In the dimension being evaluated please check which rating was given. On the line following the rating please indicate the letter(s) of the criteria that was used to determine the score. his information can be located in the AMHD LOCUS Questionnaire Booklet or in the training manual.
Composite Score
Add up the score from each dimension to determine the composite score.
Level of Care Recommendation
From the score and use of the decision tree, what is the Level of Care recommended. Write the actual name of the level (i.e. Medically Monitored
NOTE: the Level of Care recommendation may be diferent from the composite score if Independent Criteria is indicated that requires admission to a Level 5 or Level 6 service. It may also be diferent if clinical judgment is used in determining that a diferent level of care is more appropriate than what the completed LOCUS assessment recommends.
Signature spaces
Signature spaces are located at the bottom of the page on the LOCUS Recording Form. If a Mental Health (Rehab) Professional is completing the LOCUS assessment, there does not need to be a signature by a clinical supervisor.
As a mental health provider in the State of Minnesota, Deerield Behavioral Health, Inc. is granting you permission to scan this completed LOCUS Recording Form, where the dimensional scores, criteria, composite score and level of care recommendation have been documented, into your electronic medical record.