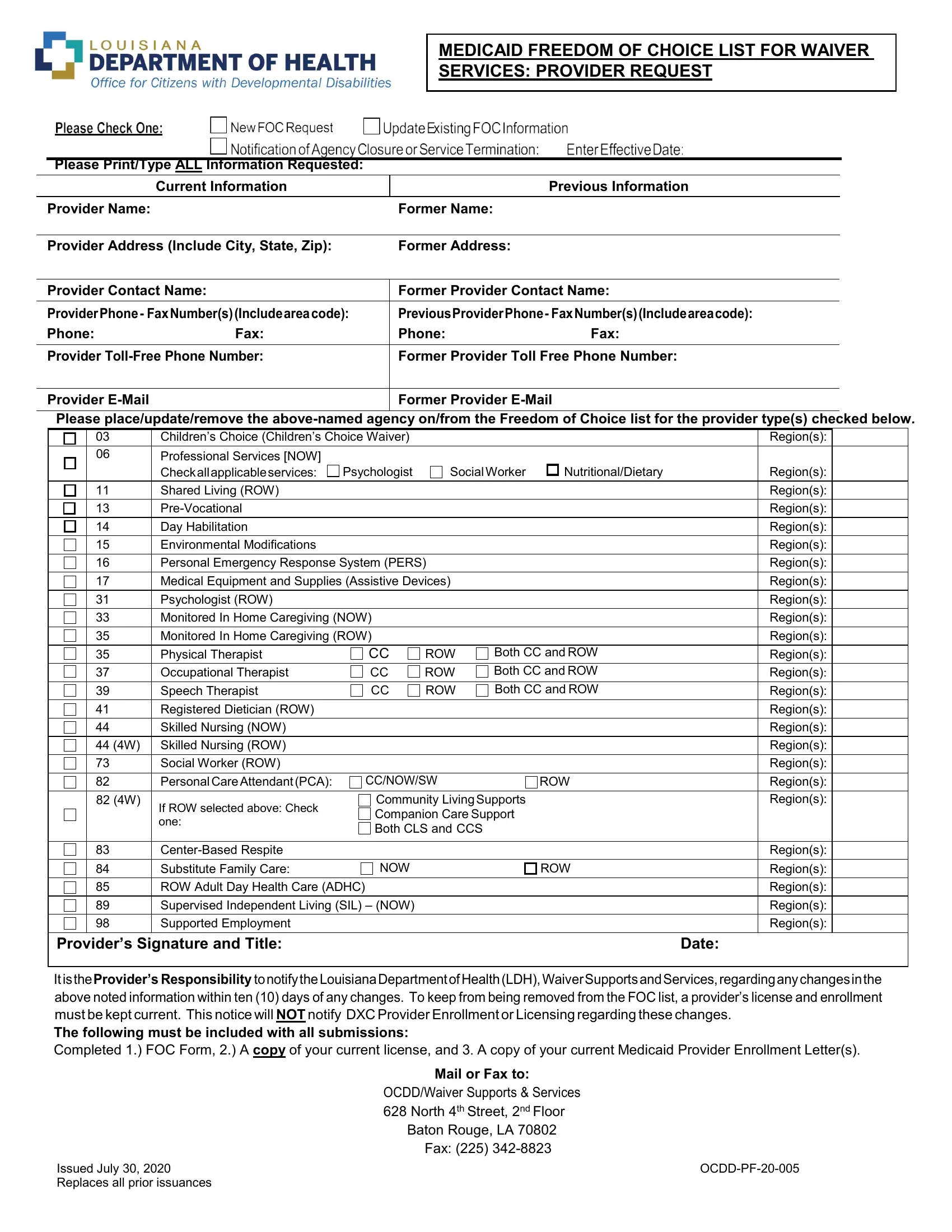
In navigating the intricacies of health care provision under Medicaid in Louisiana, providers wrestle with numerous forms and regulations, among which stands the Louisiana Medicaid Freedom of Choice List form. A critical document, it serves as a bridge between Medicaid waiver services and eligible patients, ensuring the latter's right to select from a list of qualified providers for specific healthcare services. It encompasses fields like the provider's name, contact information, and the categories of services they offer, ranging from psychological support to skilled nursing and personal care. Moreover, the form not only facilitates initial registration but also addresses any changes in provider information, emphasizing the need for timely updates to avoid removal from the Freedom of Choice list. This procedural necessity underscores a commitment to maintaining an updated roster of service options, thereby honoring the patient’s freedom of choice as enshrined in Medicaid policies. Submitting this form, complete with a current license and Medicaid Provider Enrollment Letter, is mandatory, laying the groundwork for a structured, patient-centered approach to health care provisioning within the waiver system. Issued on July 30, 2020, it supersedes all previous versions, reflecting an ongoing effort to refine and enhance the coordination between Medicaid services and beneficiary needs.
| Question | Answer |
|---|---|
| Form Name | Louisiana Medicaid Freedom of Choice List Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Form OCDD-PF-20-005 , Louisiana Medicaid Freedom of Choice List for Waiver Services Form |