
Whenever you desire to fill out ls202 form, you won't have to download any sort of applications - just try using our online PDF editor. To make our editor better and more convenient to work with, we continuously design new features, with our users' suggestions in mind. Here's what you'll need to do to begin:
Step 1: Click the "Get Form" button in the top part of this webpage to access our editor.
Step 2: The tool will allow you to change nearly all PDF documents in a range of ways. Modify it by adding personalized text, correct existing content, and include a signature - all when it's needed!
As for the fields of this particular form, here's what you want to do:
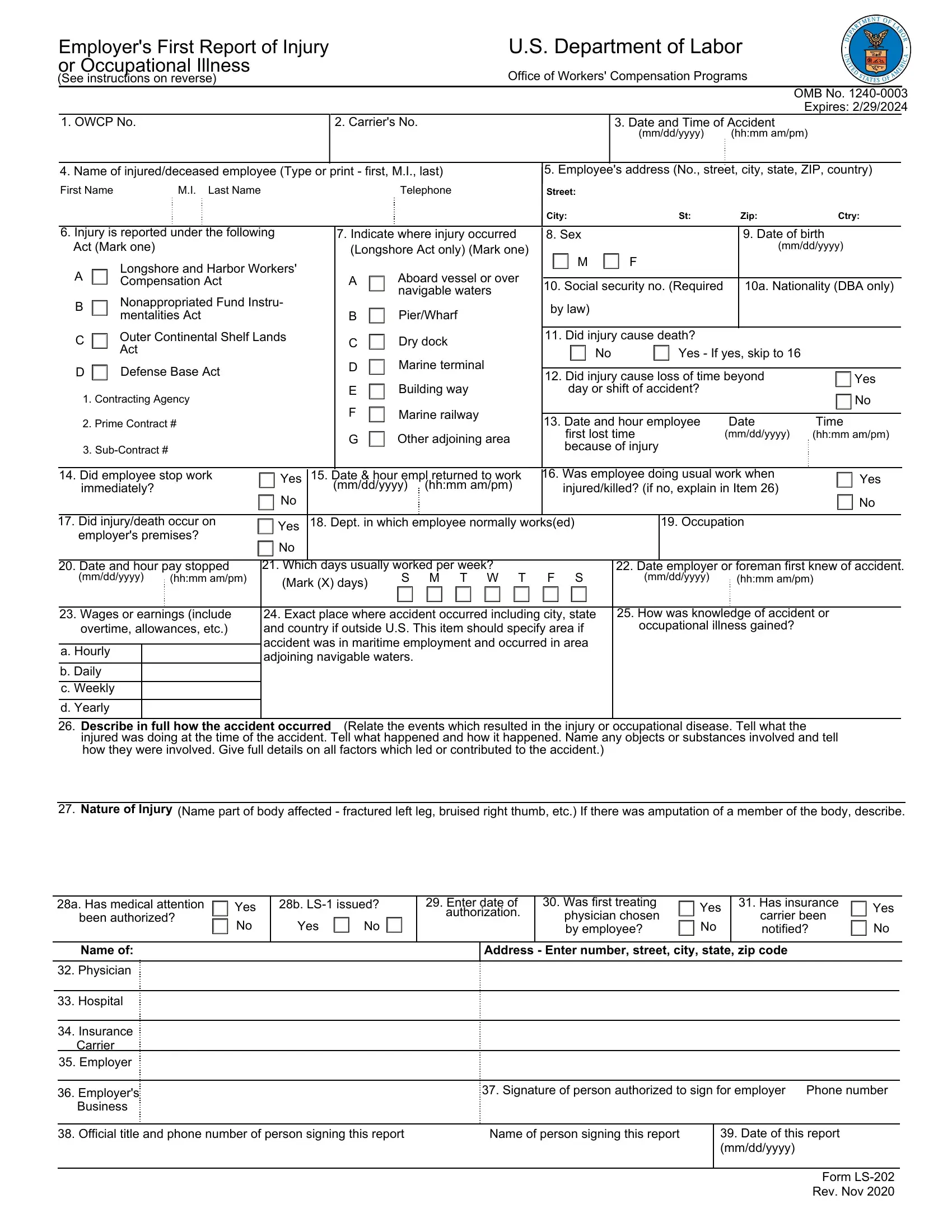
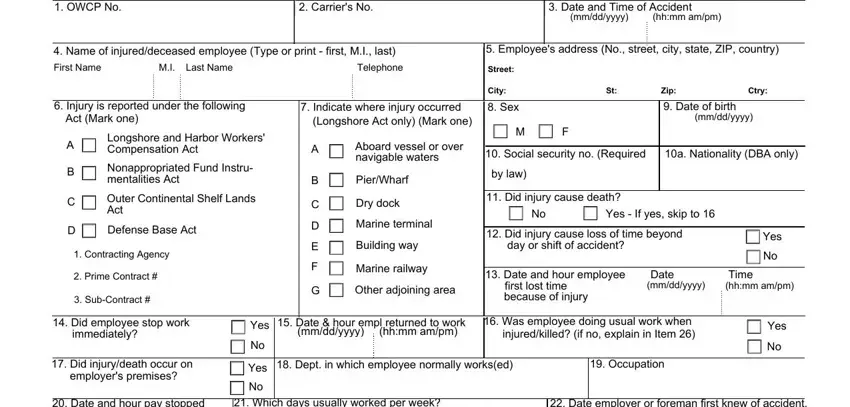
1. To start with, when filling in the ls202 form, start in the page that includes the next fields:
2. Now that the previous part is complete, it's time to include the necessary details in Date and hour pay stopped, Which days usually worked per week, mmddyyyy, hhmm ampm, Mark X days, S M T W T, Date employer or foreman first, mmddyyyy, hhmm ampm, Wages or earnings include, a Hourly, b Daily c Weekly, d Yearly, Exact place where accident, and How was knowledge of accident or in order to move forward to the next part.
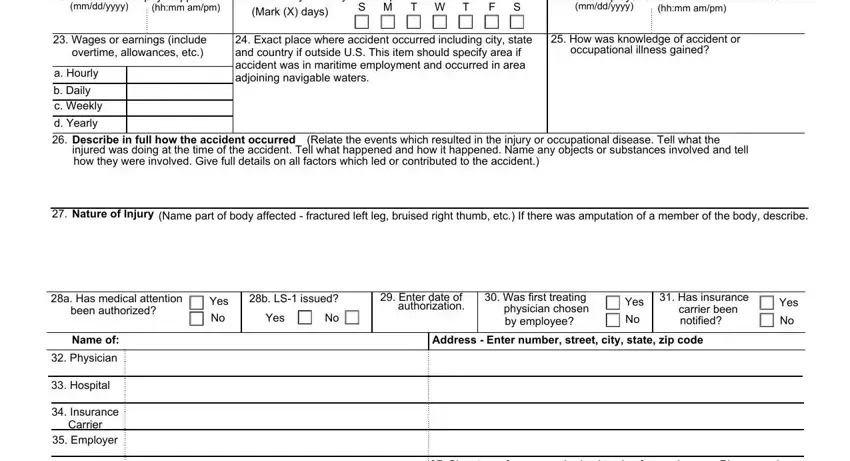
3. In this step, examine Employers, Business, Signature of person authorized to, Official title and phone number, Name of person signing this report, Date of this report mmddyyyy, and Form LS Rev Nov. Each of these are required to be filled out with greatest precision.

It is possible to make an error when filling out your Employers, thus make sure you take another look before you submit it.
Step 3: Check that your information is right and simply click "Done" to complete the process. Try a 7-day free trial account with us and get immediate access to ls202 form - readily available from your personal account page. FormsPal ensures your information privacy with a protected method that in no way saves or shares any private information provided. Be confident knowing your documents are kept confidential every time you use our editor!