 there is missing information. The MEAP crisis season runs from November 1 through May 31 therefore emergency assistance may not be available June 1 through October 31.
there is missing information. The MEAP crisis season runs from November 1 through May 31 therefore emergency assistance may not be available June 1 through October 31.
It is simple to obtain documents applying our PDF editor. Enhancing the united way lsp program form is straightforward as soon as you keep to these actions:
Step 1: You should choose the orange "Get Form Now" button at the top of the following web page.
Step 2: The file editing page is presently available. You can include information or edit existing content.
To be able to prepare the template, type in the content the application will ask you to for each of the following areas:
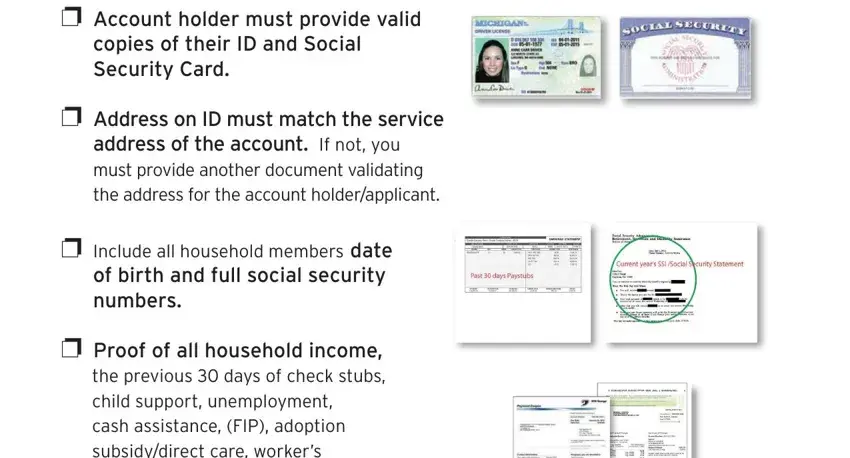
Complete the LOW INCOME SELFSUFFICIENCY PLAN LSP, APPLICATION CHECKLIST, p Must be years or older to apply, p All pages of the application, for Southeastern Michigan, p Application must be signed and, and p Account holder must provide space using the information requested by the application.
Note down any data you are required inside the area p Account holder must provide, p Address on ID must match the, p Include all household members, and p Proof of all household income.
You have to describe the rights and obligations of each side in paragraph p Include a copy of your utility, that you are seeking assistance for, and Any incomplete applications will.
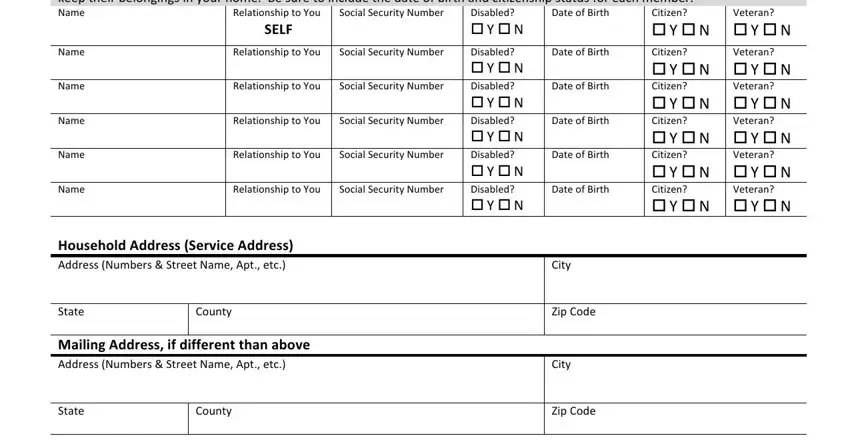
Prepare the form by taking a look at all of these fields: Name, Social Security Number, Relationship to You SELF, Household Information Attach extra, Disabled o Y o N Disabled o Y o N, Veteran o Y o N Veteran o Y o N, Disabled o Y o N, Social Security Number, Social Security Number, Social Security Number, Social Security Number, Social Security Number, Relationship to You, Relationship to You, and Relationship to You.
Step 3: Click "Done". Now you can export the PDF document.
Step 4: Be sure to get as many copies of your file as you can to stay away from future misunderstandings.
