
You may prepare magnolia prior authorization easily with the help of our online tool for PDF editing. To retain our tool on the forefront of convenience, we strive to implement user-driven features and enhancements on a regular basis. We're at all times looking for feedback - join us in revolutionizing how you work with PDF files. If you're looking to begin, here is what it will take:
Step 1: Click the orange "Get Form" button above. It will open our pdf editor so you could start filling out your form.
Step 2: With our state-of-the-art PDF editing tool, you are able to do more than simply fill out blank fields. Edit away and make your documents appear faultless with customized textual content incorporated, or modify the file's original input to perfection - all supported by the capability to add any pictures and sign it off.
It's an easy task to fill out the form adhering to our detailed guide! This is what you should do:
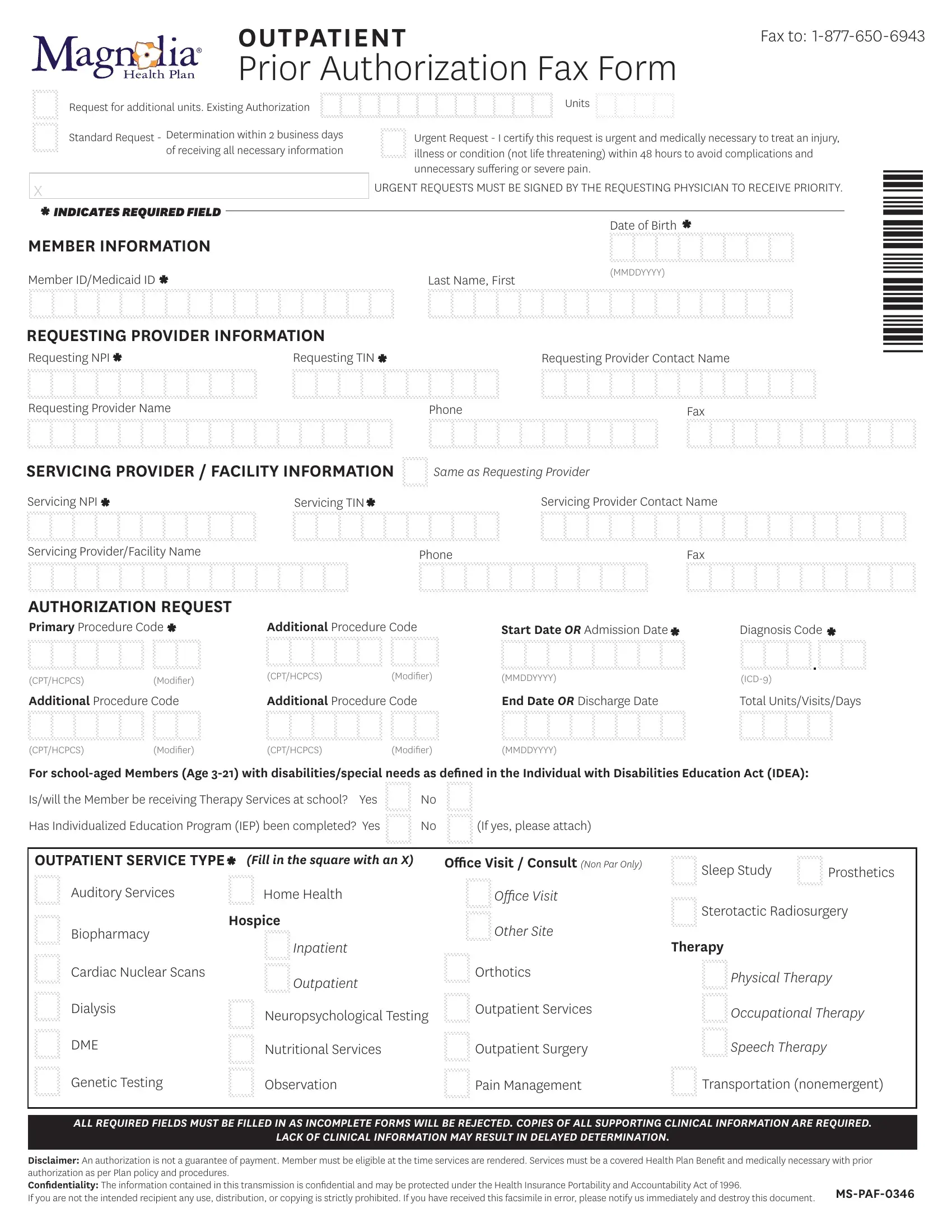
1. It is very important complete the magnolia prior authorization accurately, so take care when filling in the sections that contain all these blank fields:
2. Once the prior part is done, proceed to type in the relevant details in all these: Servicing ProviderFacility Name, Phone, Fax, AUTHORIZATION REQUEST Primary, Additional Procedure Code, Start Date OR Admission Date, Diagnosis Code, CPTHCPCS, Modiier, CPTHCPCS, Modiier, MMDDYYYY, ICD, Additional Procedure Code, and Additional Procedure Code.
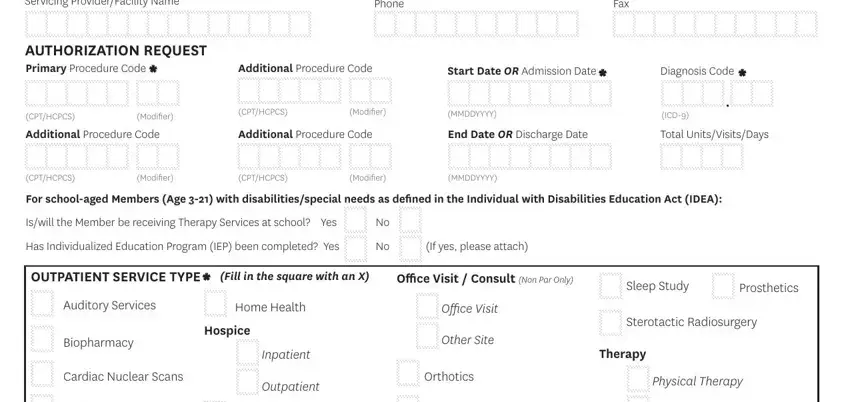
3. The following section should also be fairly easy, Neuropsychological Testing, Outpatient Services, Dialysis, DME, Occupational Therapy, Nutritional Services, Outpatient Surgery, Speech Therapy, Genetic Testing, Observation, Pain Management, Transportation nonemergent, ALL REQUIRED FIELDS MUST BE FILLED, LACK OF CLINICAL INFORMATION MAY, and Disclaimer An authorization is not - these fields needs to be filled out here.
Always be really attentive when completing Dialysis and Neuropsychological Testing, since this is where most people make a few mistakes.
Step 3: Confirm that the details are accurate and then click "Done" to progress further. Acquire your magnolia prior authorization once you sign up at FormsPal for a free trial. Readily gain access to the document inside your FormsPal cabinet, together with any modifications and changes being automatically kept! When using FormsPal, you can easily fill out documents without stressing about database breaches or records getting distributed. Our protected software helps to ensure that your private data is stored safely.