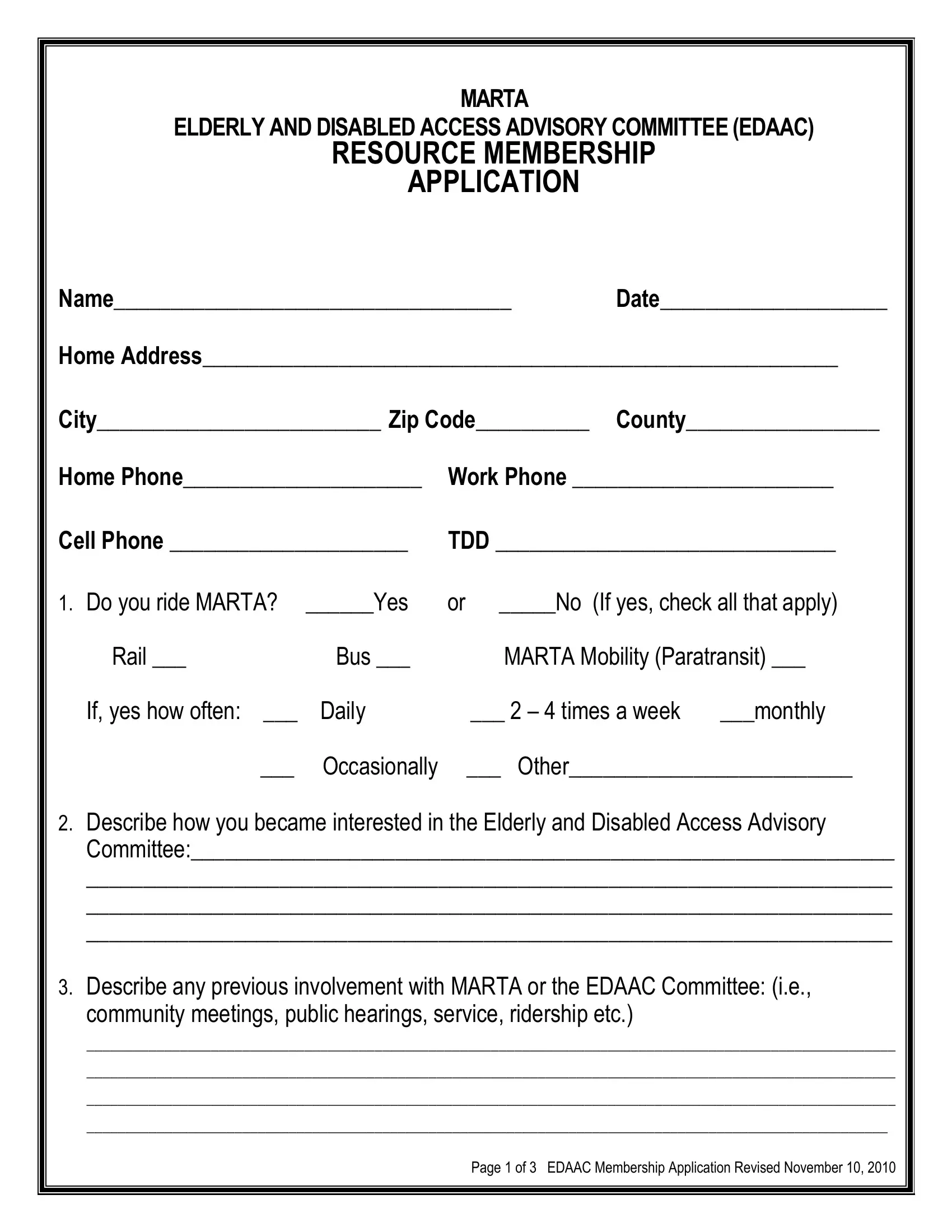
Navigating the complexities of urban transportation can present unique challenges for the elderly and individuals with disabilities, concerns that the MARTA Mobility form directly addresses. This comprehensive document serves not only as an application for those wishing to join the MARTA Elderly and Disabled Access Advisory Committee (EDAAC) but also as an invitation for community members to voice their experiences and advocate for enhanced accessibility within the public transportation realm. Applicants are asked to detail their use of MARTA services—including rail, bus, and paratransit options—thereby providing valuable insights into the practical aspects of current transit solutions and their frequency of use. Beyond this, the form encourages a deep dive into the applicant's motivations for joining the EDAAC, their history of involvement with MARTA or related community initiatives, and their associations with any organizations focused on transit, seniors, or individuals with disabilities. It further explores the applicant's personal or professional experience in working with these groups, setting a foundation for understanding the unique perspectives they might bring to the committee. The application also delves into the aspirational aspects of committee membership, asking candidates to outline their reasons for applying, the contributions they believe they can make, and their commitment to attending regular meetings—a critical component of active participation. Through this multifaceted approach, the MARTA Mobility form encapsulates a significant effort towards fostering inclusivity and accessibility in Atlanta’s transit system, underlining the vital importance of community engagement in the ongoing dialogue about public transportation services.
| Question | Answer |
|---|---|
| Form Name | Marta Mobility Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | marta mobility application pdf, marta mobility services, marta mobility application online, marta mobility application form |
MARTA
ELDERLY AND DISABLED ACCESS ADVISORY COMMITTEE (EDAAC)
RESOURCE MEMBERSHIP
APPLICATION
Name___________________________________ |
Date____________________ |
|
Home Address________________________________________________________ |
||
City_________________________ Zip Code__________ |
County_________________ |
|
Home Phone_____________________ |
Work Phone _______________________ |
|
Cell Phone _____________________ |
TDD ______________________________ |
|
1. Do you ride MARTA? ______Yes |
or _____No (If yes, check all that apply) |
|
Rail ___ |
Bus ___ |
MARTA Mobility (Paratransit) ___ |
|
If, yes how often: ___ |
Daily |
___ 2 – 4 times a week |
___monthly |
___ |
Occasionally |
___ Other_________________________ |
|
2.Describe how you became interested in the Elderly and Disabled Access Advisory Committee:______________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
3.Describe any previous involvement with MARTA or the EDAAC Committee: (i.e., community meetings, public hearings, service, ridership etc.)
Page 1 of 3 EDAAC Membership Application Revised November 10, 2010
4.Please name all community organizations in which you are currently a member that are transit related or deal with seniors and individuals with disabilities. In addition, please name all community organizations whose meetings you attend on a regular basis that are transit related or deal with seniors and individuals with disabilities.
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
5.Please give a brief synopsis of personal and/or professional experience in working with seniors and/or individuals with disabilities?
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
6.Briefly explain why you want to be a member of MARTA’s resource committee.
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
7.If you are approved to become an EDAAC resource member, what value added contributions will you bring to the Committee, the Authority, seniors and individuals with disabilities?______________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_____________________________________________________________________
8.Will you be able to commit to regular attendance at all EDAAC meetings? If not, what percentage of the 12 EDAAC Committee meetings would you be able to attend?
____100% |
____90% |
____80% |
____70% |
____60% |
____50% |
____40% |
____30% |
____20% |
____10% |
Page 2 of 3 EDAAC Membership Application Revised November 10, 2010
9.List additional information that may be important in the consideration of your application:___________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
Please append additional pages as need to tell us about other points of information that may be important in considering your application.
I WILL ABIDE BY THE RULES SET FORTH IN THE MARTA ELDERLY & DISABLED ACCESS ADVISORY COMMITTEE
SIGNATURE: ___________________________________ |
Date: _________________ |
|
|
|
|
RETURN APPLICATION:
Attention: MARTA Office of DEO
2424 PIEDMONT RD NE
ATLANTA, GA
(404)
Page 3 of 3 EDAAC Membership Application Revised November 10, 2010