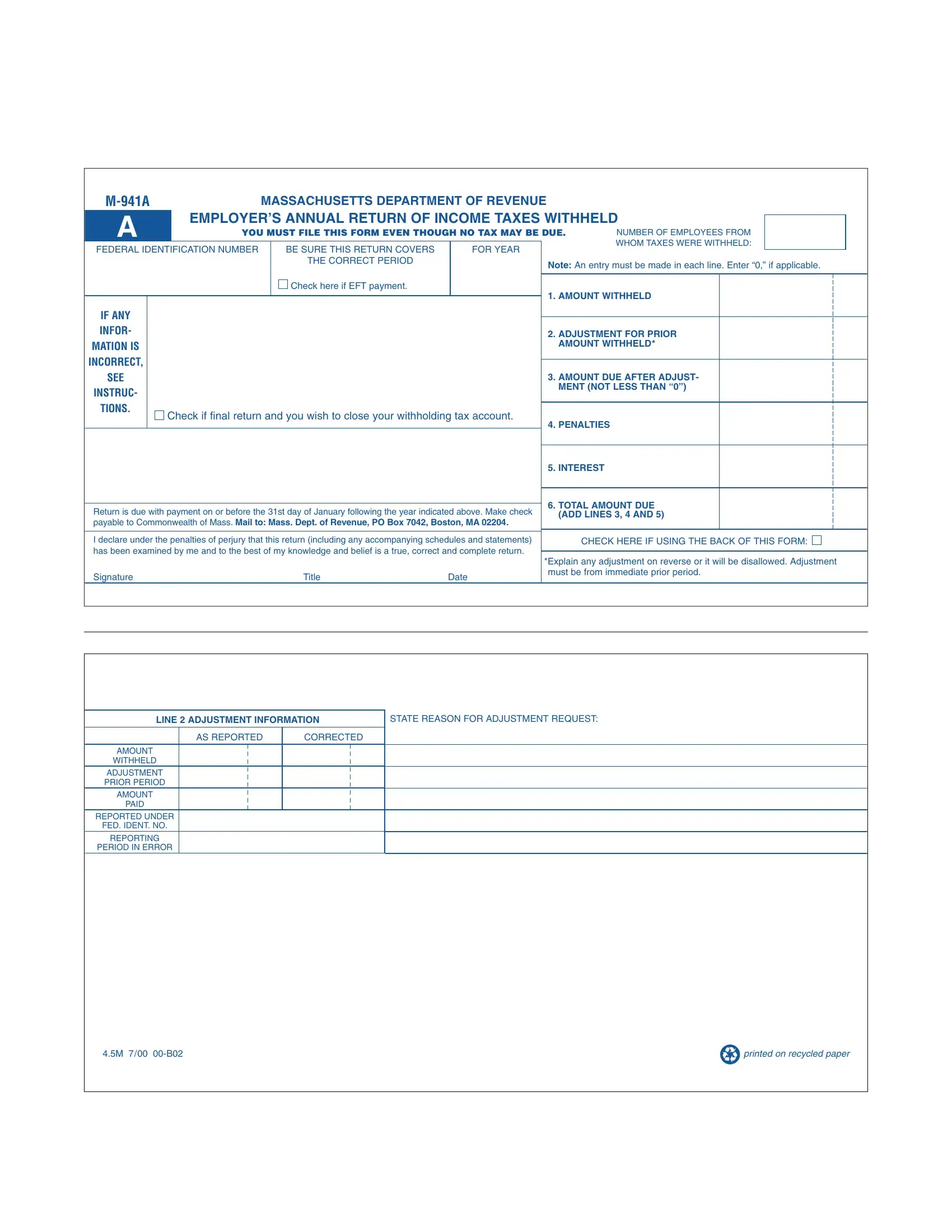
Navigating through the intricacies of tax forms can often feel daunting, yet understanding the Massachusetts M-941A form is essential for employers within the state. This form stands out as the Massachusetts Department of Revenue's way of collecting an annual return on income taxes withheld from employees. Every employer is mandated to file this form, irrespective of whether tax is due, highlighting the importance of accurate and timely submissions. With sections including the total amount withheld, adjustments for prior amounts withheld, and the computation of the amount due after adjustments, penalties, and interest, the M-941A form is comprehensive. It demands careful attention to detail—such as ensuring the correct business name, address, and federal identification number are used, and even offers the option to close your withholding tax account by checking if it's the final return. Employers must declare under penalty of perjury that the information provided is accurate, including any adjustments which must be clearly explained on the back of the form to avoid disallowance. The due date for submission with payment is the 31st day of January following the reporting year, underscoring the form's role in the annual tax cycle. Designed to ensure that income taxes withheld from employees are duly reported and paid to the Commonwealth of Massachusetts, the M-941A is a crucial document for maintaining compliance with state tax obligations.
| Question | Answer |
|---|---|
| Form Name | Massachusetts M 941A Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | mass form m 941 file online, mass ma 941 form, m941 form, withholding tax form m 941 |
|
MASSACHUSETTS DEPARTMENT OF REVENUE |
|
|
|
|
|||||||||
A |
|
EMPLOYER’S ANNUAL RETURN OF INCOME TAXES WITHHELD |
|
|
||||||||||
|
|
|
||||||||||||
|
YOU MUST FILE THIS FORM EVEN THOUGH NO TAX MAY BE DUE. |
NUMBER OF EMPLOYEES FROM |
|
|
||||||||||
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
WHOM TAXES WERE WITHHELD: |
|
|
||
FEDERAL IDENTIFICATION NUMBER |
|
BE SURE THIS RETURN COVERS |
|
FOR YEAR |
|
|||||||||
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
THE CORRECT PERIOD |
|
|
|
Note: An entry must be made in each line. Enter “0,” if applicable. |
|||||
|
|
|
|
|
|
|
|
|
||||||
|
IF INCORRECT, SEE INSTRUCTIONSCheck. DOhereNOTif EFTALTERpayment. . |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
1. AMOUNT WITHHELD |
|
|
|
||
BUSINESS |
NAME |
|
|
|
|
|
|
|
|
|
|
|
||
IF ANY |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||||
INFOR- |
|
|
|
|
|
|
|
2. ADJUSTMENT FOR PRIOR |
|
|
|
|||
BUSINESS |
ADDRESS |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
AMOUNT WITHHELD* |
|
|
|
|||||
MATION IS |
|
|
|
|
|
|
|
|
|
|
||||
INCORRECT, |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||||
CITY/SEETOWN |
|
|
|
STATE |
ZIP |
|
|
3. AMOUNT DUE AFTER ADJUST- |
|
|
|
|||
INSTRUC- |
|
|
|
|
|
|
|
|
MENT (NOT LESS THAN “0”) |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|||
TIONS. |
Check if final return and you wish to close your withholding tax account. |
|
|
|
|
|
||||||||
|
|
|
|
|
||||||||||
|
4. PENALTIES |
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. INTEREST |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
6. TOTAL AMOUNT DUE |
|
|
|
||
Return is due with payment on or before the 31st day of January following the year indicated above. Make check |
||||||||||||||
(ADD LINES 3, 4 AND 5) |
|
|
|
|||||||||||
payable to Commonwealth of Mass. Mail to: Mass. Dept. of Revenue, PO Box 7042, Boston, MA 02204. |
|
|
|
|||||||||||
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|||||||||
I declare under the penalties of perjury that this return (including any accompanying schedules and statements) |
|
CHECK HERE IF USING THE BACK OF THIS FORM: |
||||||||||||
has been examined by me and to the best of my knowledge and belief is a true, correct and complete return. |
|
|
|
|
|
|||||||||
*Explain any adjustment on reverse or it will be disallowed. Adjustment |
||||||||||||||
|
|
|
|
|
|
|
|
|
||||||
Signature |
|
|
Title |
|
Date |
must be from immediate prior period. |
||||||||
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LINE 2 ADJUSTMENT INFORMATION |
STATE REASON FOR ADJUSTMENT REQUEST: |
|
AS REPORTED |
CORRECTED |
|
AMOUNT |
|
|
WITHHELD |
|
|
ADJUSTMENT |
|
|
PRIOR PERIOD |
|
|
AMOUNT |
|
|
PAID |
|
|
REPORTED UNDER |
|
|
FED. IDENT. NO. |
|
|
REPORTING |
|
|
PERIOD IN ERROR |
|
|
4.5M 7/00 |
|
printed on recycled paper |