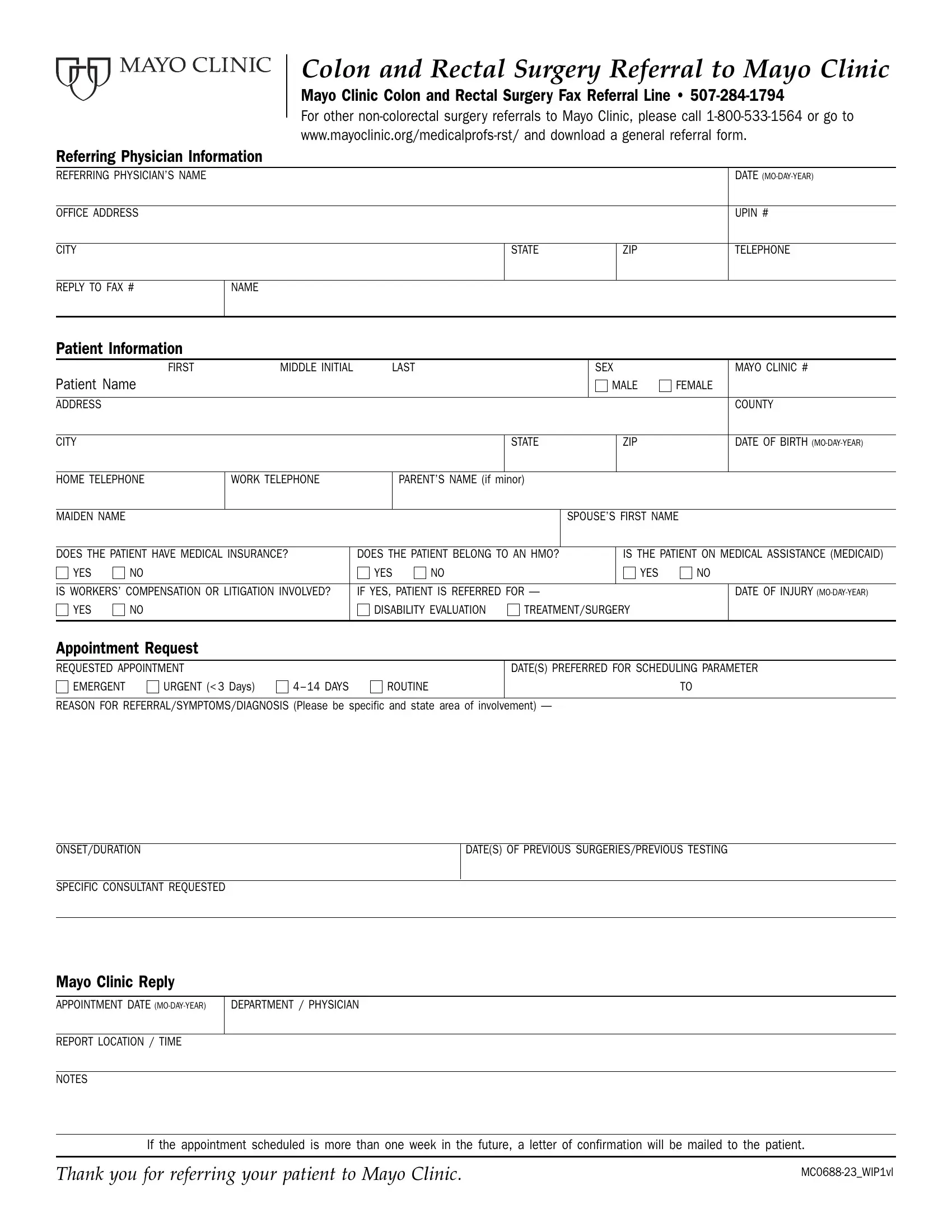
When medical professionals or patients face complex medical needs, especially concerning colon and rectal surgery, accessing specialized care is crucial. Among the reputable institutions providing such specialized services, the Mayo Clinic stands out. Those seeking referral for Colon and Rectal Surgery at Mayo Clinic must navigate through a specific procedure underpinned by a detailed referral form. This essential document encompasses several sections, including detailed instructions for the referring physician, encompassing the physician’s contact information, patient information noting key demographics and insurance details, the urgency of the appointment, and the specific nature of the referral, including symptoms, diagnosis, and any prior treatments or surgeries relevant to the case at hand. The form also inquires about whether the patient is involved in workers’ compensation or litigation related to their condition, which could influence the approach to treatment or evaluation. Additionally, the referral form leaves space for preferred dates for scheduling the appointment, highlighting the Mayo Clinic's commitment to accommodating patient needs. The referral process culminates with a section dedicated to the Mayo Clinic's reply, ensuring clear communication regarding the appointment details. This systematic approach not only facilitates a streamlined referral process for colon and rectal surgery at one of America's top medical institutions but also exemplifies the Mayo Clinic's dedication to providing accessible, high-quality patient care.
| Question | Answer |
|---|---|
| Form Name | Mayo Clinic Referral Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | mayo clinic referral forms, mayo clinic fax referral form, mayo clinic referral sheet pediatric orthop, mayo clinic referral form |