

You'll be able to fill in printable food stamp application ohio instantly with our online editor for PDFs. To maintain our editor on the cutting edge of convenience, we work to put into action user-driven features and improvements on a regular basis. We are at all times pleased to get suggestions - help us with revolutionizing how you work with PDF forms. This is what you'd have to do to get going:
Step 1: Access the PDF inside our tool by clicking the "Get Form Button" in the top section of this webpage.
Step 2: This editor allows you to change nearly all PDF forms in many different ways. Improve it with your own text, adjust original content, and place in a signature - all when you need it!
When it comes to blanks of this particular PDF, here is what you should do:
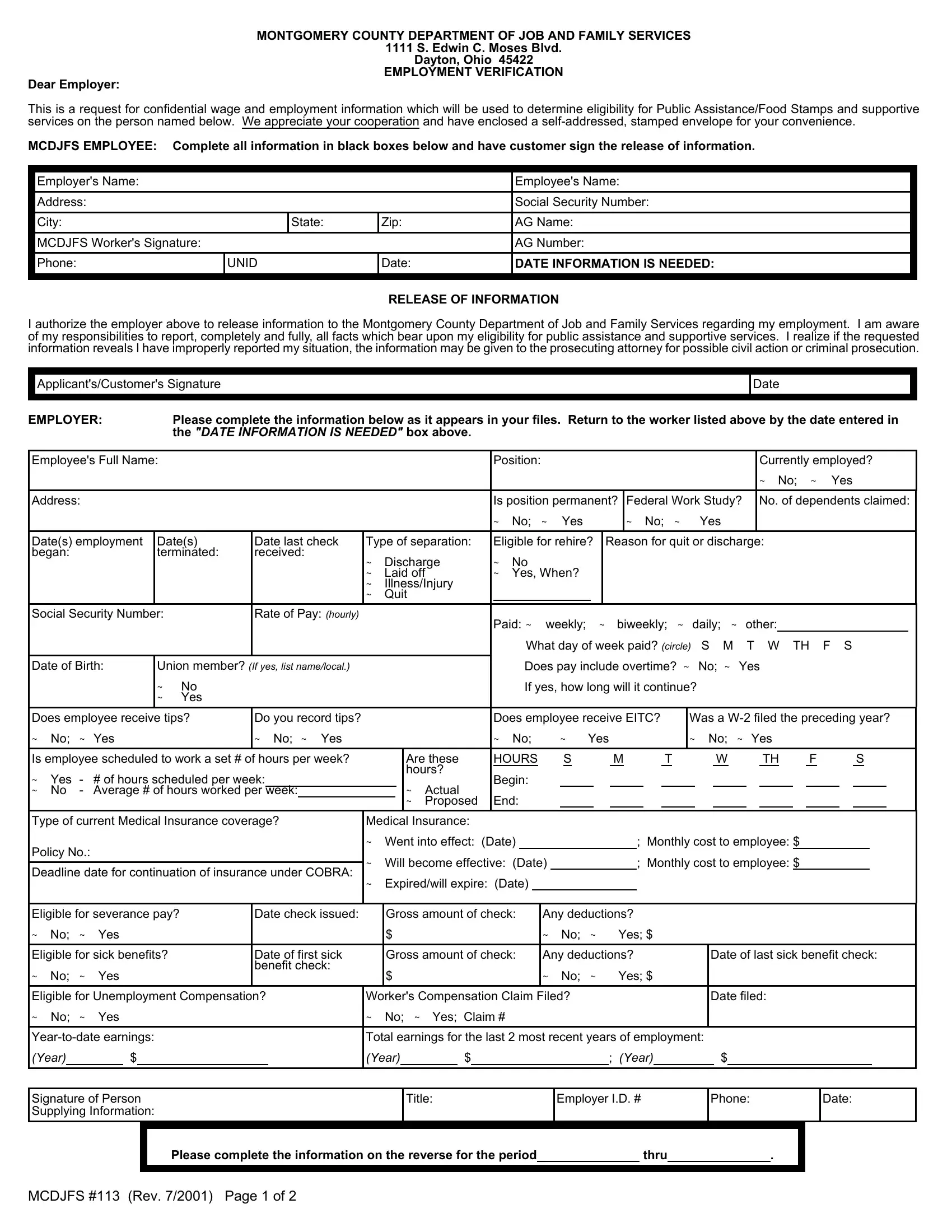
1. The printable food stamp application ohio involves particular details to be typed in. Make sure the subsequent blank fields are filled out:
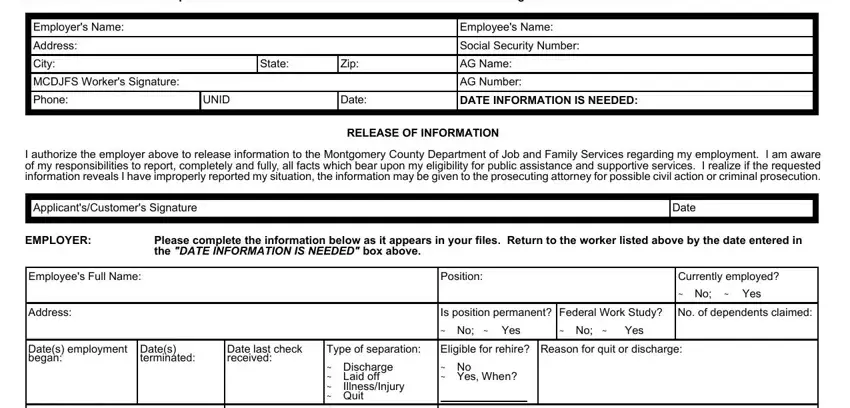
2. When this section is filled out, go to type in the relevant details in all these - Signature of Person Supplying, Please complete the information on, and MCDJFS Rev Page of.

Many people generally make errors when filling in Signature of Person Supplying in this section. Be sure you go over everything you enter here.
Step 3: Right after you have reviewed the details in the fields, simply click "Done" to finalize your form. Create a 7-day free trial account at FormsPal and acquire instant access to printable food stamp application ohio - readily available inside your personal cabinet. FormsPal ensures your data privacy with a secure method that never records or distributes any sort of private information provided. Feel safe knowing your paperwork are kept safe when you use our editor!