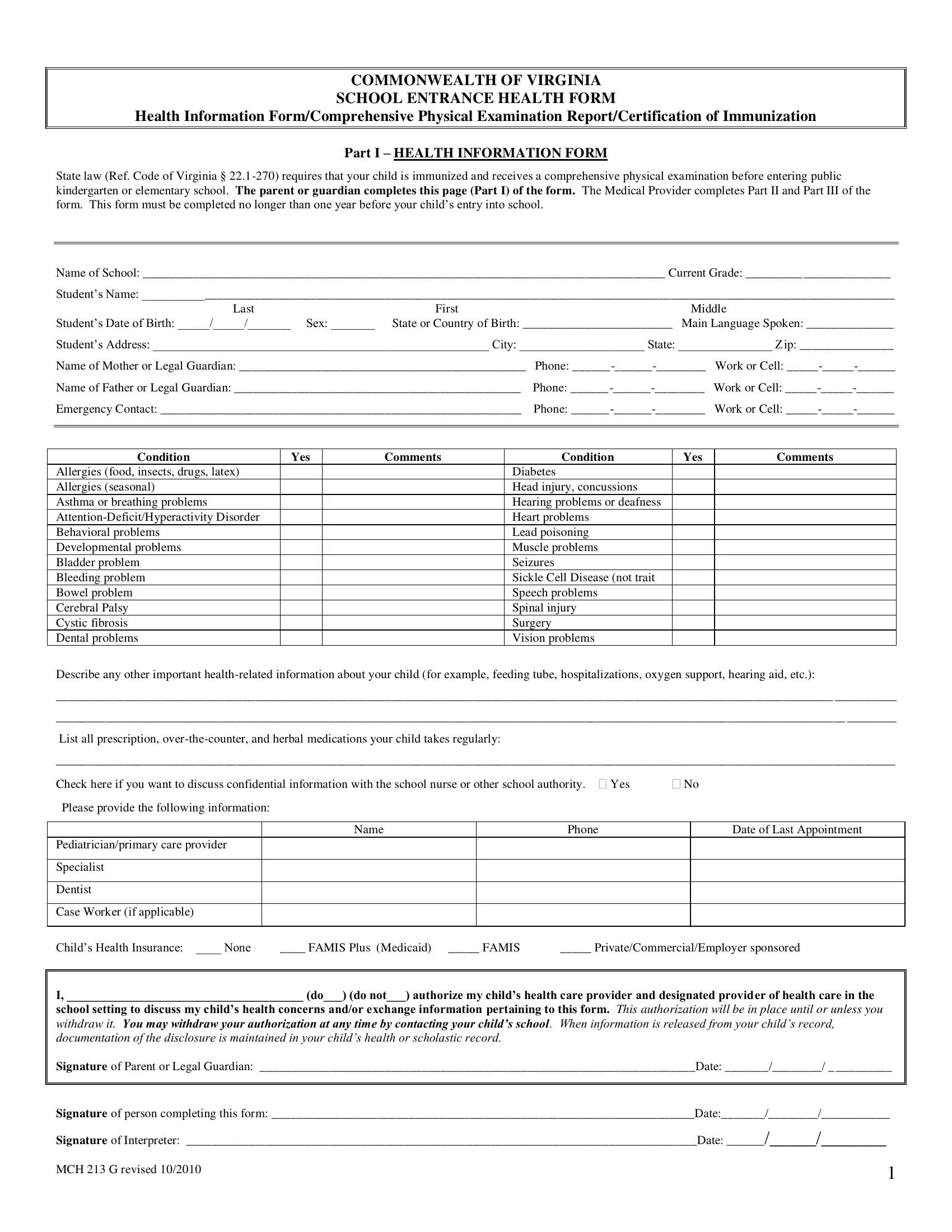
Navigating the entrance into public kindergarten or elementary school in Virginia necessitates a thorough preparation in terms of health requirements, a primary aspect of which is encapsulated in the MCH 213 G form. This comprehensive document serves as a tri-partite tool, incorporating Health Information Form, Comprehensive Physical Examination Report, and Certification of Immunization, each section designed to fulfill the state's health prerequisites for school attendees. The form, updated in October 2010, demands that a child's immunization records be current and includes a detailed physical examination before their school entry, aligning with Virginia Code § 22.1-270. Parents or guardians are tasked with completing the initial segment, which captures vital health information and consent for medical discussions with school authorities. The subsequent sections, aimed at documenting immunizations and the physical examination, are strictly for healthcare providers to fill out, ensuring the student meets the minimum health standards for school attendance. Critical in this process is the presentation of a child's allergy status, existing conditions, and overall health readiness, pivotal for crafting a supportive educational environment. Additionally, the form delves into exemptions and conditional enrollments, guidelines that cater to specific health-related stipulations, ultimately safeguarding both the child's wellbeing and public health interests within the school setting.
| Question | Answer |
|---|---|
| Form Name | Mch 213 G Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | health forms, virginia school physical form, virginia school entrance health form 2021, virginia school entrance health form |