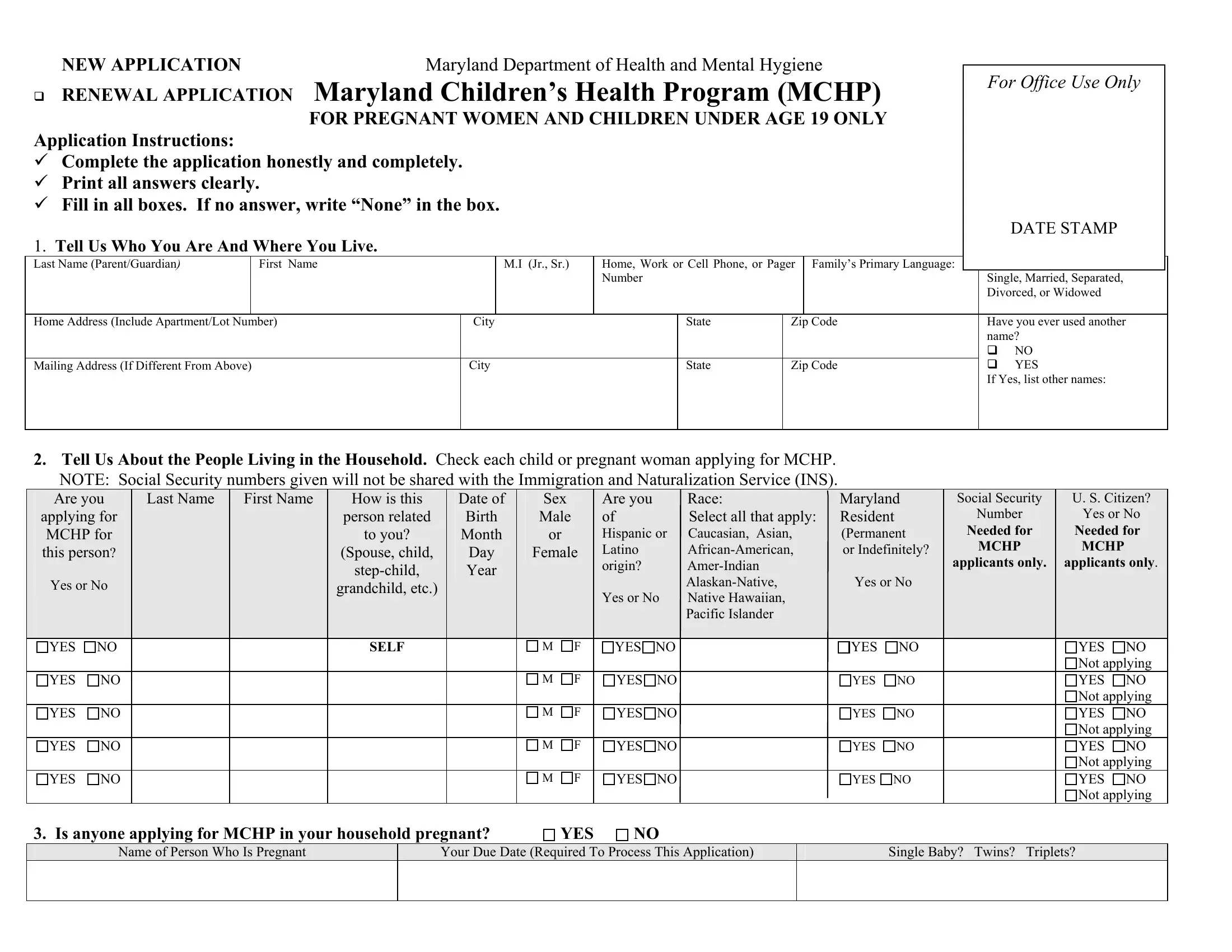
Embarking on the path to securing health coverage for pregnant women and children under the age of 19, the Maryland Children's Health Program (MCHP) application form serves as a critical first step. Designed by the Maryland Department of Health and Mental Hygiene, this form is a gateway for applicants to provide necessary information that determines eligibility for health benefits. Applicants are guided through a series of questions aimed at gathering comprehensive data on household composition, financial situation, and specific healthcare needs. Whether it's a new application or a renewal, the form solicits details such as personal identification, residency, income, and any other health insurance coverages, emphasizing the importance of truthful and complete responses. Beyond aligning with procedural necessities, the form encapsulates a commitment to confidentiality and outlines applicant rights and responsibilities, underscoring Maryland’s dedication to a transparent and fair process. Each section, meticulously crafted, reminds applicants of the underlying objective: to extend crucial health benefits to those in need, ensuring that children and pregnant women receive the care they deserve.
| Question | Answer |
|---|---|
| Form Name | Mchp Application Online Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | md woman renewal online, application mchp online, mchp application, application online mchp |
NEW APPLICATION |
Maryland Department of Health and Mental Hygiene |
|
|
For Office Use Only |
|||
RENEWAL APPLICATION |
Maryland Children’s Health Program (MCHP) |
||
|
|||
|
FOR PREGNANT WOMEN AND CHILDREN UNDER AGE 19 ONLY |
|
Application Instructions:
Complete the application honestly and completely.
Print all answers clearly.
Fill in all boxes. If no answer, write “None” in the box.
DATE STAMP
1.Tell Us Who You Are And Where You Live.
Last Name (Parent/Guardian) |
|
First Name |
|
M.I (Jr., Sr.) |
Home, Work or Cell Phone, or Pager |
Family’s Primary Language: |
|
|
Marital Status (Circle One): |
|
|||
|
|
|
|
|
Number |
|
|
|
|
Single, Married, Separated, |
|||
|
|
|
|
|
|
|
|
|
|
|
Divorced, or Widowed |
||
|
|
|
|
|
|
|
|
|
|
|
|
||
Home Address (Include Apartment/Lot Number) |
City |
|
State |
Zip Code |
Have you ever used another |
||||||||
|
|
|
|
|
|
|
|
|
|
|
name? |
||
|
|
|
|
|
|
|
|
|
|
|
|
NO |
|
Mailing Address (If Different From Above) |
|
City |
|
State |
Zip Code |
|
YES |
||||||
|
|
|
|
|
|
|
|
|
|
|
If Yes, list other names: |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2.Tell Us About the People Living in the Household. Check each child or pregnant woman applying for MCHP.
NOTE: Social Security numbers given will not be shared with the Immigration and Naturalization Service (INS).
|
Are you |
|
Last Name |
First Name |
|
How is this |
|
|
Date of |
|
|
Sex |
|
|
|
Are you |
|
Race: |
Maryland |
|
|
Social Security |
|
|
U. S. Citizen? |
|
|||
|
applying for |
|
|
|
|
person related |
|
|
Birth |
|
|
Male |
|
|
|
of |
|
Select all that apply: |
Resident |
|
|
|
Number |
|
|
Yes or No |
|
||
|
MCHP for |
|
|
|
|
to you? |
|
|
Month |
|
|
or |
|
|
|
Hispanic or |
Caucasian, Asian, |
(Permanent |
|
|
Needed for |
|
|
Needed for |
|
||||
|
this person? |
|
|
|
|
(Spouse, child, |
|
|
Day |
|
|
Female |
|
|
Latino |
|
or Indefinitely? |
|
|
MCHP |
|
|
MCHP |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
applicants only. |
|
|
applicants only. |
|
|||||||||||
|
|
|
|
|
|
|
|
|
Year |
|
|
|
|
|
|
origin? |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Yes or No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes or No |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
grandchild, etc.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes or No |
Native Hawaiian, |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pacific Islander |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
NO |
|
|
|
SELF |
|
|
|
|
M |
F |
|
YES |
NO |
|
YES |
NO |
|
|
|
|
YES |
NO |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Not applying |
||
|
YES |
NO |
|
|
|
|
|
|
|
|
|
M |
F |
|
YES |
NO |
|
YES |
NO |
|
|
|
|
YES |
NO |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Not applying |
||
|
YES |
NO |
|
|
|
|
|
|
|
|
|
M |
F |
|
YES |
NO |
|
YES |
NO |
|
|
|
|
YES |
NO |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Not applying |
||
|
YES |
NO |
|
|
|
|
|
|
|
|
|
M |
F |
|
YES |
NO |
|
YES |
NO |
|
|
|
|
YES |
NO |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Not applying |
||
|
YES |
NO |
|
|
|
|
|
|
|
|
|
M |
F |
|
YES |
NO |
|
YES NO |
|
|
|
|
YES |
NO |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Not applying |
||
3. Is anyone applying for MCHP in your household pregnant? |
|
YES |
|
NO |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
Name of Person Who Is Pregnant
Your Due Date (Required To Process This Application)
Single Baby? Twins? Triplets?
4.Tell Us If Anyone Applying For MCHP (Child or Pregnant Woman) Has Any Unpaid Medical Bills For Services Received In The Three (3) Months Prior to the Month of Application. Examples of unpaid medical bills would include doctor’s visits, hospitalization, medical tests, prescriptions, equipment, etc.
|
|
|
4B. Tell us who received medical care and when. |
|
|
4A. Do you want MCHP to help with these unpaid bills? |
YES |
NO |
Name |
Month/Year |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5.Tell Us If Anyone Applying For MCHP Has Other Medical Expenses, for which a third party may be responsible. Fill out the following information if anyone applying for MCHP has medical expenses that are a result of an accident, job injury or malpractice, or is expecting to receive an accident settlement, trust fund, inheritance or other money or property.
Name of Injured Person |
Date of Accident/Injury |
|
|
Name and Address of Other Persons or Companies That May Be Responsible |
|
|
|
Money or Property Expected |
Name, Address and Telephone No. of Attorney Involved |
|
|
6. If The Child Applying For MCHP Is Not Eligible For Free Medical Care
Would you (the parent or guardian of the applicant) be willing to pay $46.00 - $58.00 premium payment each month to cover all children in the household for health insurance
coverage through MCHP Premium? |
YES |
NO |
7A. Does Anyone Applying For MCHP Have |
YES |
NO |
|
|
|||||
If Yes, answer the following: |
|
|
|
|
|
|
|
|
|
Name of Policy Holder ______________________________________________________ |
Name of Person(s) covered ______________________________________________ |
||||||||
|
|
Name |
|
|
|
|
|
|
|
Insurance Company Name ___________________________________________________ |
Policy Number _______________________ |
|
|
||||||
Group#_______________________________ |
Effective Date ___________________________ |
End Date _______________________________ |
|||||||
|
|
||||||||
7B. Have you dropped |
|
||||||||
YES |
NO |
|
|
|
|
|
|
|
|
If yes, please tell us when and why coverage was dropped: |
|
|
|||||||
Changed Employer |
Terminated From Job |
Employer dropped coverage |
|
COBRA Coverage Ended |
No Longer Needed |
Quit Job |
|||
Cost |
Moved Out of Service Area Of Employer’s Health Plans |
Dropped Limited Benefit Insurance (Vision, Dental, Not Hospital) |
Other: ______________ |
||||||
|
|
|
|
|
|
|
|
|
|
8.Tell Us About Family Income.
A. Earned Income. List any wages, tips, commissions, earnings or money from
We don’t count income from other adults in the household (grandparents, aunts, and uncles).
Name of Employed
Person
Name of Employer
Address of Employer
Street, City, State, Zip Code
Telephone
Number
Gross Amount Paid
(before taxes)
Each Pay Period
How Often Paid?
weekly |
biweekly |
monthly |
2x monthly |
quarterly |
annually |
Job
Start Date
Job
End Date
Student
Status
(Full or
B. Unearned Income. List any other income received such as alimony, child support, pension, Social Security, income received from renting property to others and benefits (retirement, strike benefits, unemployment, veterans, workers compensation). Include
Person Receiving Income |
Type (For Benefits, Include Claimant ID #) |
Gross Amount Received |
How Often? |
|
|
|
|
|
|
|
|
C . If you didn’t list any income in 8A. or 8B., how do you get food and shelter?_________________________________________________________________________
9A. Tell Us If You Pay For Child Care While You Are Working. This expense lowers the amount of income we count and may help you become eligible.
Name of Child Care Provider or Day Care Center |
|
Telephone # |
|
Name(s) of Child(ren) Cared For |
|
Your Cost |
|
|
Who Pays For This Child? |
|||||
|
|
|
|
|
|
|
|
|
$ |
PER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
PER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Do you have Purchase of Care Services/Vouchers through the Department of Social Services? |
YES |
NO |
|
|
|
|
|
|||||||
9B. Tell Us If You Pay Child Support Or Alimony. These expenses lower the amount of income we count and may help you become eligible. |
|
|
|
|||||||||||
Name of Person In Your Household Who Is Paying |
|
Name of Person Outside Your Household Who Is |
|
Amount Paid |
|
|
|
How Often? |
||||||
|
Child Support or Alimony |
|
|
Receiving These Payments |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10. Other Information |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Maryland Children’s Health Program would like to know how you found out about |
If anyone in your household is not registered to vote, would they be interested in |
|||||||||||||
our program. |
|
|
|
|
|
receiving voter registration forms? |
YES |
NO |
How Many?_______ |
|||||
Friend |
Family |
School |
Community Organization |
|
|
|
|
ALREADY REGISTERED |
||||||
Doctor/Health Care Professional |
Advertisement |
Other _________ |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|

Here are your rights and responsibilities under the Maryland Children’s Health Program.
Please read these carefully before signing below.
Health Care Benefits I know I have the right to request and, if found eligible, to receive MCHP benefits based on policies and standards established under Maryland law. If I am applying as a pregnant woman, I understand that abortion is not covered.
Confidentiality I understand that the information I have given is confidential. I agree that medical information about my children or me can be released when the law allows.
Social Security Number (SSN) I understand that providing the SSNs of MCHP applicants is required and that providing the social security numbers of other household members and MCHP Premium applicants is voluntary. I will not be penalized if the SSNs of household members who are not applying for MCHP or the SSNs of MCHP Premium applicants are not provided. SSNs will not be shared with Immigration and Naturalization Services (INS), and will only be used to help check the information about income and insurance coverage and to help maintain eligibility files. If I do not have a SSN and want to apply for one, I understand that my case manager will help me.
Personal and Financial Information I agree to the release of personal and financial information from this application form to the agencies determining eligibility. I give permission for officials of the Maryland Children’s Health Program to verify all information on this form. I understand I may be asked to provide additional information.
Third Party Payments And Cooperation With Quality Control Review I understand that I am required by law to assign to the State all rights to medical support and other third party payments (hospital and medical benefits) and to cooperate with the State’s Medical Assistance quality control review process including verification of all information pertinent to the determination of eligibility.
Reporting Changes I have a responsibility to report all changes that might affect eligibility within ten (10) days of the change. Examples of changes I must report are changes in number of people in the household, address, income, employment and pregnancy. I can report changes in person, by telephone, or by mail to my case manager at my local health department or at the Department of Health and Mental Hygiene.
Rights I know that this application will be considered without regard to race, color, sex, age, handicap, religion,
national origin or political belief. I know that I may request a hearing if I believe the State of Maryland in processing my application has made an error or if I feel I have been discriminated against. I have the right to appeal any action taken by the Department. If I ask for a hearing, my case manager can help me put my request in writing. At my hearing, I can speak for myself or have someone else represent me. I have a right to a written notice of all decisions affecting my eligibility.
Please sign this statement.
I certify that the information I have provided above is true to the best of my knowledge and I give permission for the State of Maryland to make any necessary contacts to check my statements. I have read the list of my rights and responsibilities. I know that I can be penalized if I knowingly give false information. I certify that the children and pregnant woman for whom I am applying are U.S. citizens or lawful immigrants or are applying for emergency services only.
This application must be signed by a pregnant or
Signature: |
|
Date: ______ |
_________________ |
|
|
|
|
|
|
PLEASE PRINT NAME