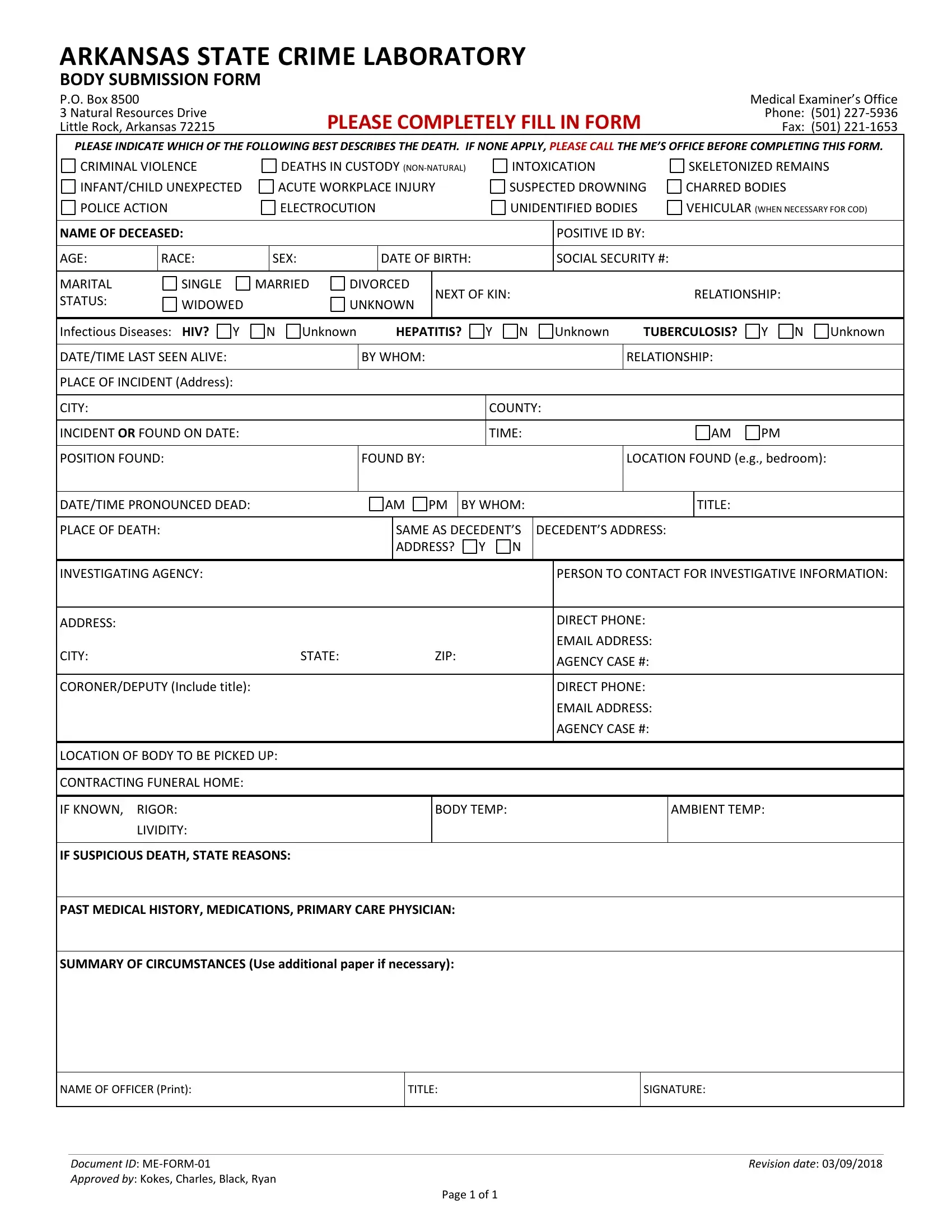
Within the vast expanse of forensic science and legal procedure, documents play a pivotal role in stitching together narratives from fragments of evidence. The Arkansas State Crime Laboratory's Body Submission Form, known as ME Form 01, embodies a comprehensive approach to gathering vital information during the sensitive early stages of post-mortem investigations. This form serves as a bridge between the scene of an incident and the analytical rigor of the laboratory, demanding meticulous detail about the deceased, ranging from personal identifiers such as name, age, and race to the circumstances surrounding their death, including the date, time, and location of the incident. Furthermore, it delves into specific aspects of the case, prompting the entering of data on whether the death was due to natural causes, an accident, suicide, or involves suspicion of foul play. The inclusion of details regarding infectious diseases, marital status, and the involvement of law enforcement agencies underscores the multifaceted nature of death investigations, demanding a careful balance between scientific inquiry and sensitivity towards the deceased and their families. This form not only facilitates a systematic approach to the examination of the deceased but also plays a critical role in ensuring that all relevant details are considered, providing a foundational document that aids in the pursuit of truth and justice within the framework of forensic science.
| Question | Answer |
|---|---|
| Form Name | Me Form 01 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | arkansas crime lab forms, arkansas state crime lab forms, arkansas state crime lab submission forms, arkansas state crime lab submission form |
