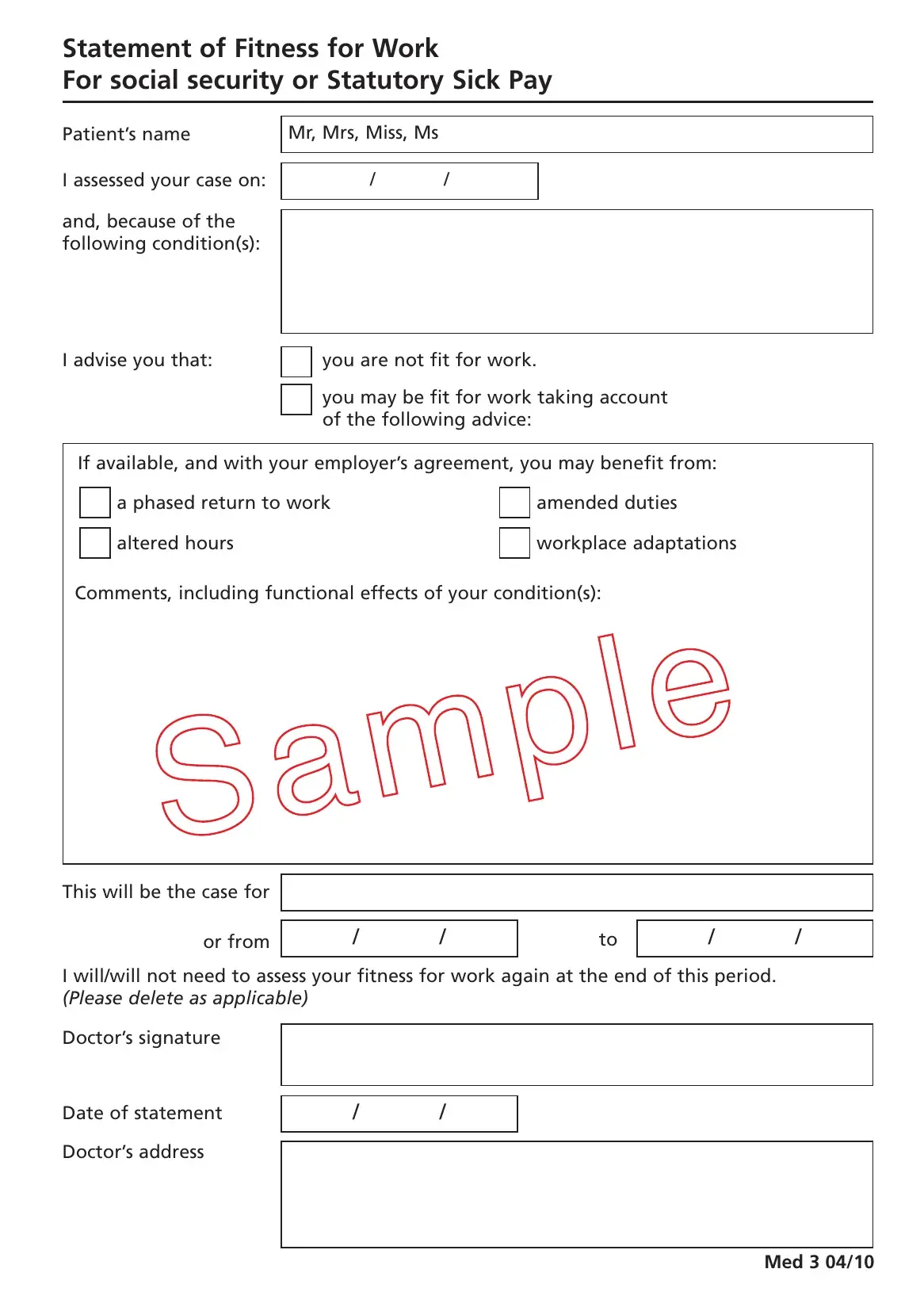
The Med 3 form, known officially as the Statement of Fitness for Work, serves a crucial role in bridging the gap between health care professionals and employment obligations for individuals facing health challenges. This document, vital for patients who find themselves unable to perform their job duties due to physical or psychological conditions, creates a structured pathway for discussing and documenting an individual’s work capacity. Through a clear layout, including sections for the patient’s personal information, a detailed assessment date, and the specific condition(s) affecting their fitness for work, the form delineates whether a person is completely unfit for work or may return under adjusted conditions. It introduces the possibility of a tailored return to work through amended duties, altered hours, or workplace adaptations, directly engaging with the employer's capacity to accommodate these needs. Furthermore, the form includes a section for doctors to note the expected duration of the work impact and whether a follow-up assessment is necessary, offering a timeline for both the patient and employer. The form ends with mandatory fields for the doctor's signature, the date of the statement, and the doctor's address, ensuring the document’s validity and traceability. Designed with both the patient's welfare and the employer's operational requirements in mind, the Med 3 form is indispensable for managing health-related absences in the workforce.
| Question | Answer |
|---|---|
| Form Name | Med 3 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | med3 form, med 3 form, fit note template uk pdf, unique id med 3 01 17 |
Statement of Fitness for Work
For social security or Statutory Sick Pay
Patient’s name |
Mr, Mrs, Miss, Ms |
|
|
|
|
|
|
|
|
|
|
I assessed your case on: |
/ |
/ |
|
and, because of the |
|
|
|
|
|
|
|
|
|
|
|
following condition(s): |
|
|
|
|
|
|
|
I advise you that: |
|
you are not fit for work. |
|||||
|
|
|
|
you may be fit for work taking account |
|||
|
|
|
|
||||
|
|
|
|
||||
|
|
|
|
of the following advice: |
|
||
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
If available, and with your employer’s agreement, you may benefit from: |
|||||||
|
|
a phased return to work |
|
|
amended duties |
||
|
|
|
|
||||
|
|
altered hours |
|
|
|
|
workplace adaptations |
|
|
|
|
|
|
||
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
Comments, including functional effects of your condition(s): |
|||||||
|
|
|
|
|
|
|
|
This will be the case for
or from |
/ |
/ |
to |
/ |
/ |
|
|
|
|
|
|
I will/will not need to assess your fitness for work again at the end of this period. (Please delete as applicable)
Doctor’s signature
Date of statement Doctor’s address
//
Med 3 04/10