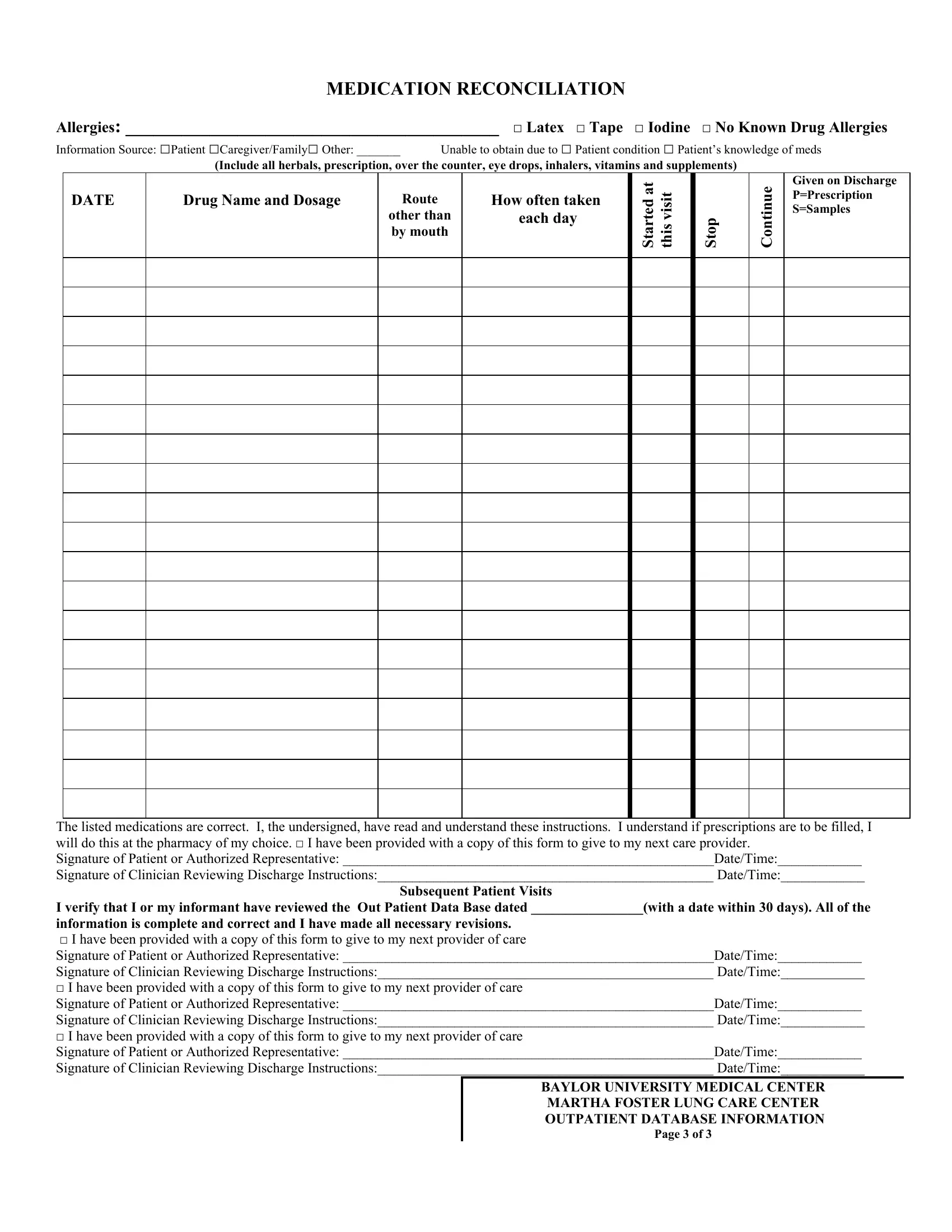
In the landscape of medical care, the Med Rec And Schedule form stands as a cornerstone in ensuring a seamless transition and communication between healthcare providers, patients, and their caregivers. This comprehensive document plays a critical role in medication reconciliation, a process integral to patient safety and effective healthcare delivery. It meticulously records allergies, including common ones to latex, tape, and iodine, as well as any known drug allergies, ensuring personalized care and prevention of adverse reactions. The form bridges communication gaps by identifying the source of information, be it from the patient, caregiver, or otherwise, and provides space for documenting all forms of medication, including herbals, over-the-counter medications, prescriptions, eye drops, inhalers, vitamins, and supplements. By detailing medication names, dosages, routes of administration other than oral, and frequencies, it offers a clear medication management plan. It also facilitates tracking medication changes, specifying whether drugs were started, continued, or stopped at the visit, and if they were given on discharge, including whether these were prescriptions or samples. Signatures from both the patient or authorized representative and the clinician reviewing discharge instructions underscore the form's role in verifying the accuracy and understanding of information, further extending its relevance to subsequent patient visits. This form, utilized by institutions like the Baylor University Medical Center Martha Foster Lung Care Center, exemplifies the meticulous attention to detail required in outpatient care, highlighting its crucial role in ensuring continuity of care and patient well-being.
| Question | Answer |
|---|---|
| Form Name | Med Rec And Schedule Template Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | medication reconciliation form pdf, printable blank medication forms, sjhhc medication reconciliation form template printable, city of forest park ohio reconciliation form |