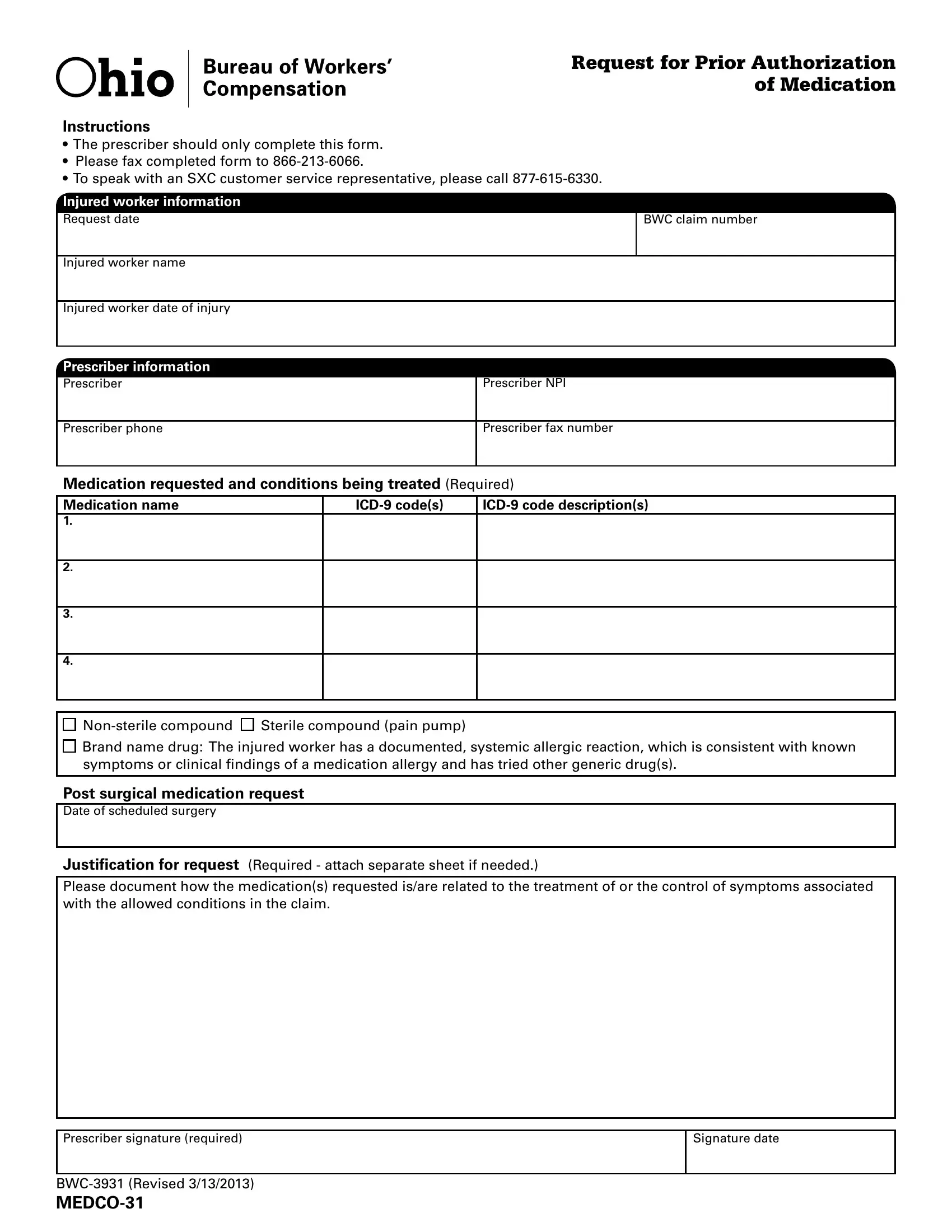
The Medco 31 form serves a crucial function in the medical and insurance fields, streamlining the process for prior authorization of medication. Designed specifically for use by prescribers, it ensures that individuals injured on the job receive timely access to necessary medications related to their workers' compensation claim. Prescribers are tasked with completing this document, including detailed sections on injured worker information, the prescriber's details, and the intricate specifics of the medication requested along with the conditions being treated. Essential fields include the injured worker’s name, claim number, and the date of injury, alongside the prescriber's contact information and qualifications. Another critical section mandates the listing of medication names, corresponding ICD-9 codes, and the precise reasons for the medication request, which could range from treating direct injury aftermath to managing pain via non-sterile or sterile compounds and brand name drugs under specific conditions such as documented allergies. The form also accommodates requests for post-surgical medication, requiring justification that links the medication directly to the worker's injury or surgical recovery. A mandatory requirement for the prescriber's signature underscores the accountability and authenticity of the request, aligning with the protocol to fax the completed document to a designated number for processing. Such a systematized approach not only expedites necessary medical treatment but also ensures the comprehensive documentation of medication requests within the framework of workers' compensation claims.
| Question | Answer |
|---|---|
| Form Name | Medco 31 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | ICD-9, amerigroup authorization form, amerigroup prior authorization, Justification |
Request for Prior Authorization of Medication
Instructions
•The prescriber should only complete this form.
•Please fax completed form to
•To speak with an SXC customer service representative, please call
Injured worker information
Request date
BWC claim number
Injured worker name
Injured worker date of injury
Prescriber information
Prescriber
Prescriber NPI
Prescriber phone
Prescriber fax number
Medication requested and conditions being treated (Required)
Medication name |
1.
2.
3.
4.
Brand name drug: The injured worker has a documented, systemic allergic reaction, which is consistent with known symptoms or clinical indings of a medication allergy and has tried other generic drug(s).
Post surgical medication request
Date of scheduled surgery
Justification for request (Required - attach separate sheet if needed.)
Please document how the medication(s) requested is/are related to the treatment of or the control of symptoms associated with the allowed conditions in the claim.
Prescriber signature (required)
Signature date