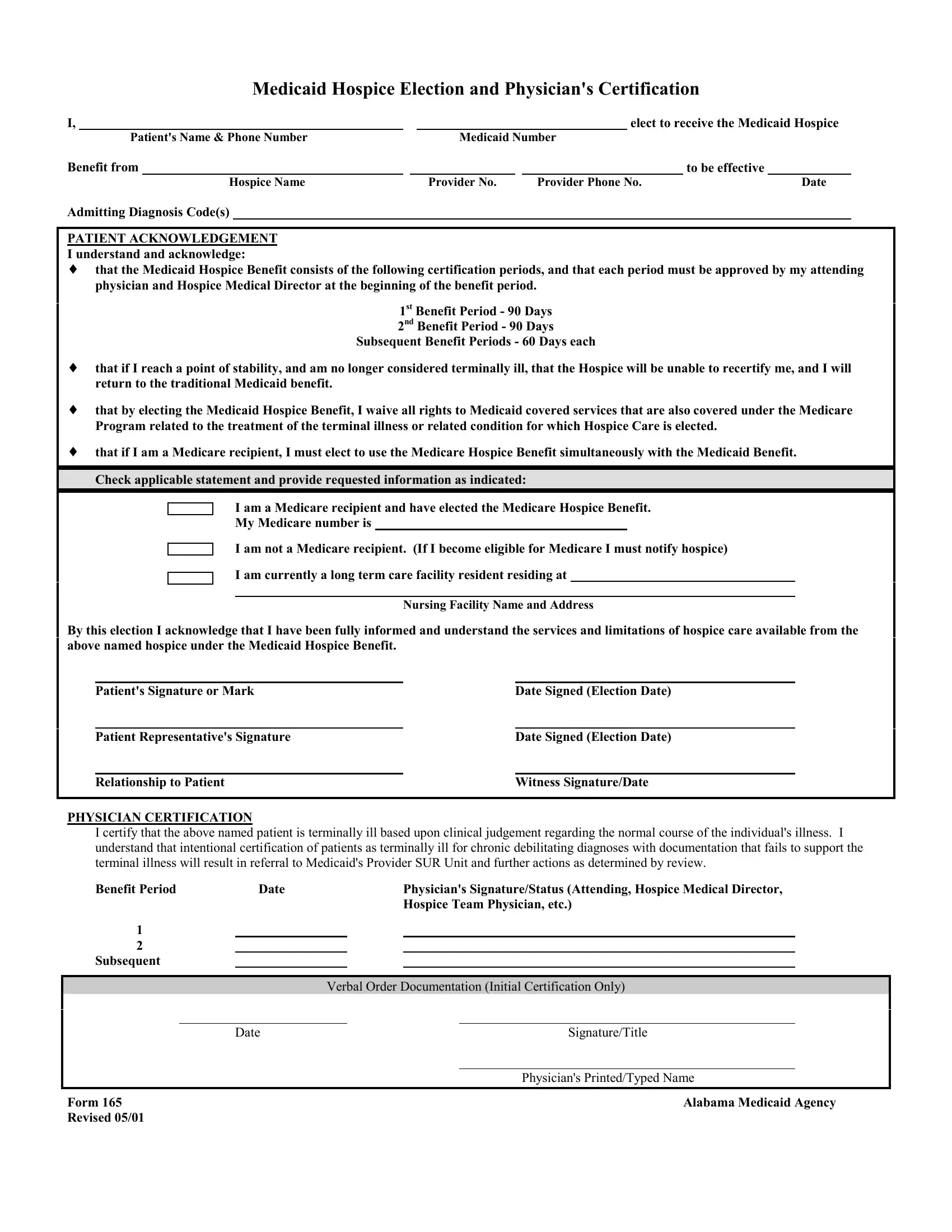
When faced with the challenging journey of hospice care, navigating the realm of healthcare benefits can seem daunting. Among the crucial documents in this process is the Medicaid 165 form, officially titled the Medicaid Hospice Election and Physician's Certification. This form serves as a vital link for patients choosing to receive hospice care under Medicaid, clearly laying out the terms of the hospice benefit, including the certification periods required for care continuation, and the patient's acknowledgment of these terms. It comprehensively captures a patient's intent to elect hospice care, detailing patient information, hospice provider details, and admitting diagnosis codes, ensuring that the election for hospice benefit is well documented and acknowledged. Moreover, it addresses the intersection of Medicaid and Medicare benefits, outlining the need for patients who are Medicare recipients to elect the Medicare Hospice Benefit concurrently with Medicaid, if applicable. Importantly, the form facilitates the physician's certification that the patient in question is terminally ill, a certification that carries significant weight as it determines the patient's eligibility for hospice care under Medicaid. This form is a cornerstone in the hospice care process, encapsulating the election, understanding, and medical verification needed to access compassionate care in the face of terminal illness.
| Question | Answer |
|---|---|
| Form Name | Medicaid Form 165 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 3D 2c 8 Hospice Election Form 165 medicaid hospice alabama form |
Medicaid Hospice Election and Physician's Certification
I, |
|
|
|
|
|
|
elect to receive the Medicaid Hospice |
|||
|
Patient's Name & Phone Number |
|
|
Medicaid Number |
|
|
||||
Benefit from |
|
|
|
|
|
|
to be effective |
|||
|
|
Hospice Name |
|
|
Provider No. |
|
Provider Phone No. |
|
Date |
|
Admitting Diagnosis Code(s)
PATIENT ACKNOWLEDGEMENT
I understand and acknowledge:
♦that the Medicaid Hospice Benefit consists of the following certification periods, and that each period must be approved by my attending physician and Hospice Medical Director at the beginning of the benefit period.
1st Benefit Period - 90 Days
2nd Benefit Period - 90 Days
Subsequent Benefit Periods - 60 Days each
♦that if I reach a point of stability, and am no longer considered terminally ill, that the Hospice will be unable to recertify me, and I will return to the traditional Medicaid benefit.
♦that by electing the Medicaid Hospice Benefit, I waive all rights to Medicaid covered services that are also covered under the Medicare Program related to the treatment of the terminal illness or related condition for which Hospice Care is elected.
♦that if I am a Medicare recipient, I must elect to use the Medicare Hospice Benefit simultaneously with the Medicaid Benefit. Check applicable statement and provide requested information as indicated:
I am a Medicare recipient and have elected the Medicare Hospice Benefit.
My Medicare number is
I am not a Medicare recipient. (If I become eligible for Medicare I must notify hospice)
I am currently a long term care facility resident residing at
Nursing Facility Name and Address
By this election I acknowledge that I have been fully informed and understand the services and limitations of hospice care available from the above named hospice under the Medicaid Hospice Benefit.
Patient's Signature or Mark
Patient Representative's Signature
Relationship to Patient
Date Signed (Election Date)
Date Signed (Election Date)
Witness Signature/Date
PHYSICIAN CERTIFICATION
I certify that the above named patient is terminally ill based upon clinical judgement regarding the normal course of the individual's illness. I understand that intentional certification of patients as terminally ill for chronic debilitating diagnoses with documentation that fails to support the terminal illness will result in referral to Medicaid's Provider SUR Unit and further actions as determined by review.
Benefit Period |
Date |
|
Physician's Signature/Status (Attending, Hospice Medical Director, |
||||
|
|
|
|
|
Hospice Team Physician, etc.) |
||
1 |
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
Subsequent |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
Verbal Order Documentation (Initial Certification Only) |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
Signature/Title |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician's Printed/Typed Name |
|
|
|
|
|
|
|
||
Form 165 |
|
|
|
|
Alabama Medicaid Agency |
||
Revised 05/01 |
|
|
|
|
|
|
|