
In case you need to fill out dd 2807 1, you won't need to download any applications - just make use of our PDF tool. We at FormsPal are committed to giving you the ideal experience with our editor by regularly adding new capabilities and upgrades. Our tool has become a lot more intuitive as the result of the newest updates! At this point, editing PDF files is a lot easier and faster than before. This is what you would want to do to start:
Step 1: Simply click the "Get Form Button" above on this webpage to access our pdf file editor. There you will find everything that is required to work with your document.
Step 2: With the help of this state-of-the-art PDF file editor, it is possible to do more than just fill out blank form fields. Try each of the functions and make your forms appear sublime with customized text added in, or tweak the file's original content to excellence - all that comes along with the capability to insert stunning photos and sign the document off.
This document will need particular data to be typed in, so be sure to take your time to provide precisely what is expected:
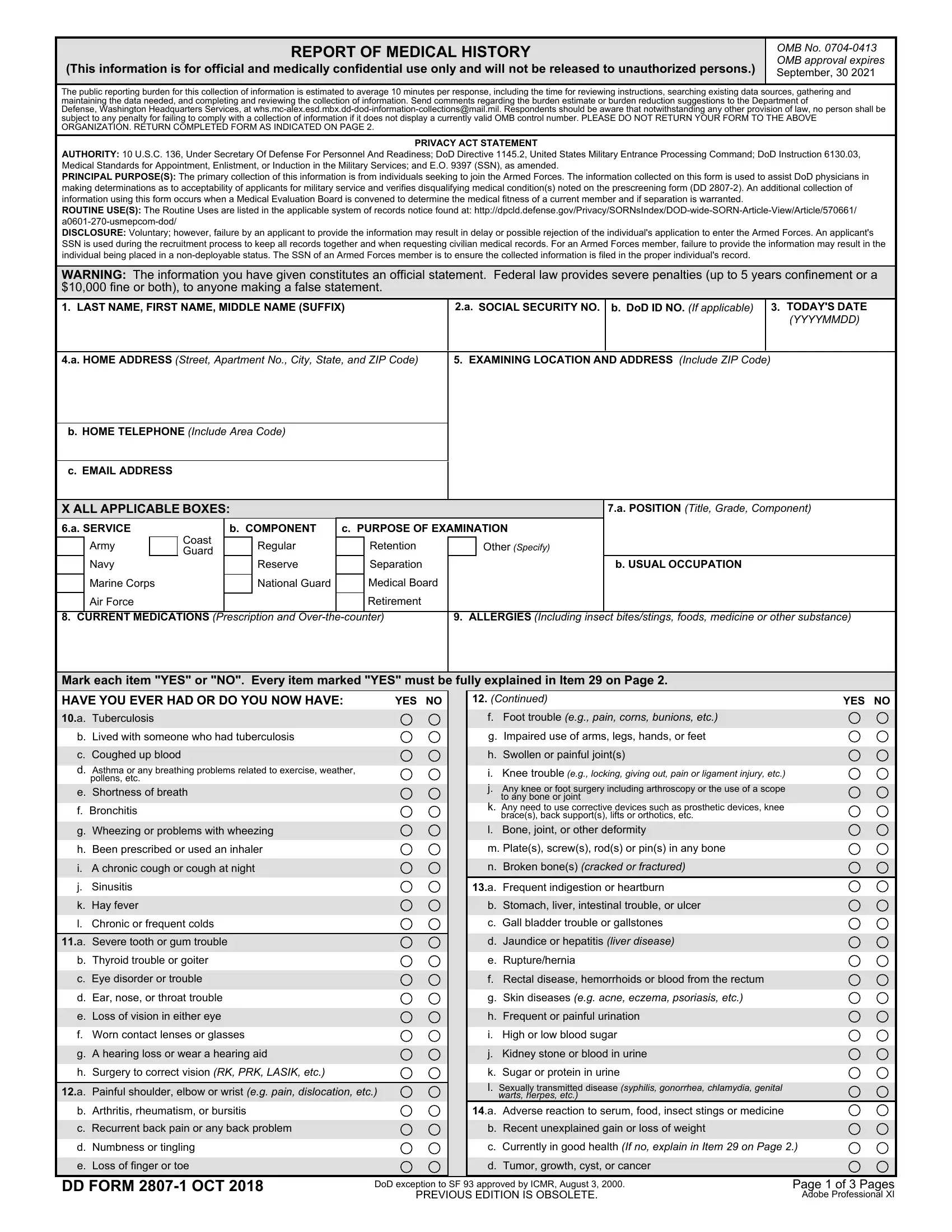
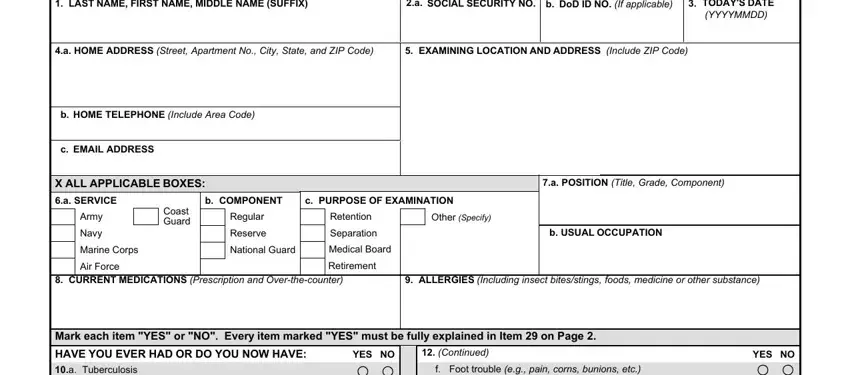
1. Firstly, when filling out the dd 2807 1, start with the section that has the subsequent blanks:
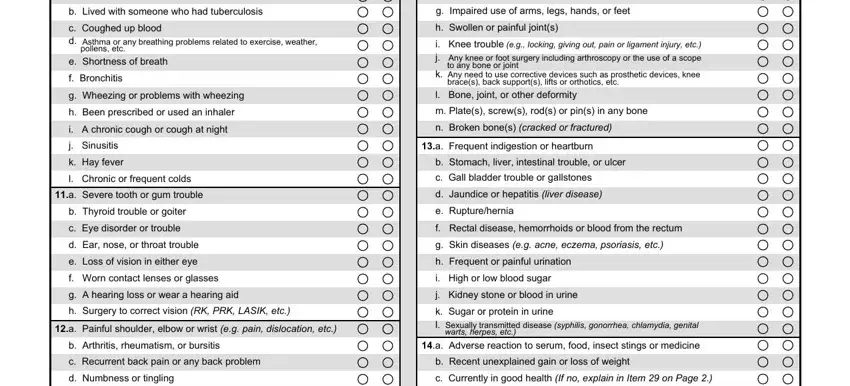
2. Just after completing this step, head on to the next part and fill out the essential details in all these fields - Mark each item YES or NO Every, b Lived with someone who had, pollens etc, e Shortness of breath f Bronchitis, a Severe tooth or gum trouble, b Thyroid trouble or goiter c Eye, a Painful shoulder elbow or wrist, b Arthritis rheumatism or bursitis, f Foot trouble eg pain corns, to any bone or joint, braces back supports lifts or, l Bone joint or other deformity m, a Frequent indigestion or heartburn, b Stomach liver intestinal trouble, and warts herpes etc.
3. The following segment should also be fairly straightforward, b Arthritis rheumatism or bursitis, DD FORM OCT, b Recent unexplained gain or loss, DoD exception to SF approved by, PREVIOUS EDITION IS OBSOLETE, and Page of Pages Adobe Professional - all of these blanks needs to be filled in here.

It's easy to make errors while filling in the b Arthritis rheumatism or bursitis, and so be sure to take another look before you decide to send it in.
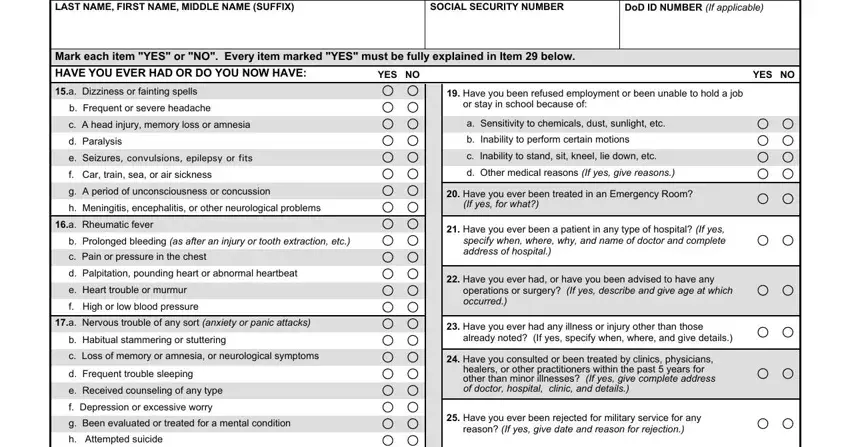
4. The next subsection comes with these particular form blanks to fill out: LAST NAME FIRST NAME MIDDLE NAME, SOCIAL SECURITY NUMBER, DoD ID NUMBER If applicable, Mark each item YES or NO Every, YES NO, Have you been refused employment, YES NO, b Frequent or severe headache c A, a Rheumatic fever, b Prolonged bleeding as after an, a Nervous trouble of any sort, b Habitual stammering or, or stay in school because of a, Have you ever been treated in an, and If yes for what.
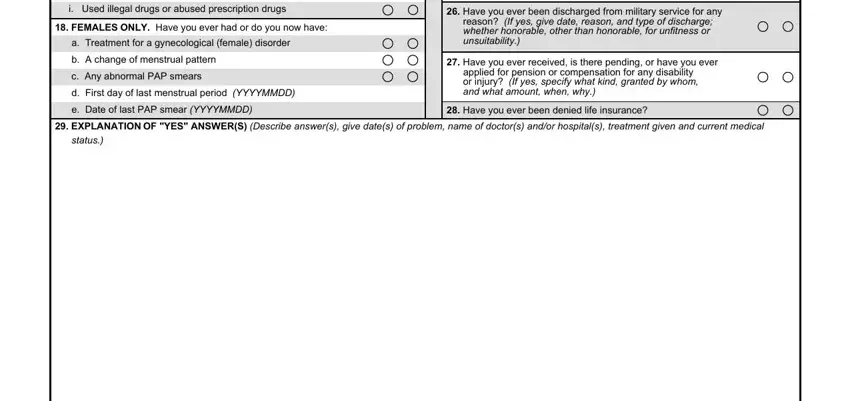
5. This very last stage to complete this form is pivotal. Be certain to fill in the mandatory blanks, and this includes b Habitual stammering or, FEMALES ONLY Have you ever had or, a Treatment for a gynecological, Have you ever been discharged, reason If yes give date reason and, Have you ever received is there, applied for pension or, Have you ever been denied life, EXPLANATION OF YES ANSWERS, and status, before finalizing. Neglecting to do so may generate an incomplete and probably unacceptable paper!
Step 3: Once you've looked again at the information you given, simply click "Done" to conclude your document creation. Join FormsPal now and easily get dd 2807 1, prepared for download. All alterations made by you are saved , helping you to change the form at a later time as required. FormsPal offers secure form editor without personal information record-keeping or distributing. Feel comfortable knowing that your data is secure here!