Are you a medical professional looking for a streamlined and secure system to facilitate referrals? Look no further! A well-designed, automated referral form can reduce inefficiencies, improve data accuracy and security, and allow your organization to focus on caring for the health of your patients. In this blog post, we will explore why investing in an electronic medical referral form is essential; how it works; what benefits it provides to all parties involved; as well as some tips on how best to utilize them. Read on to learn more about the advantages of having an advanced referral form system in place!
| Question | Answer |
|---|---|
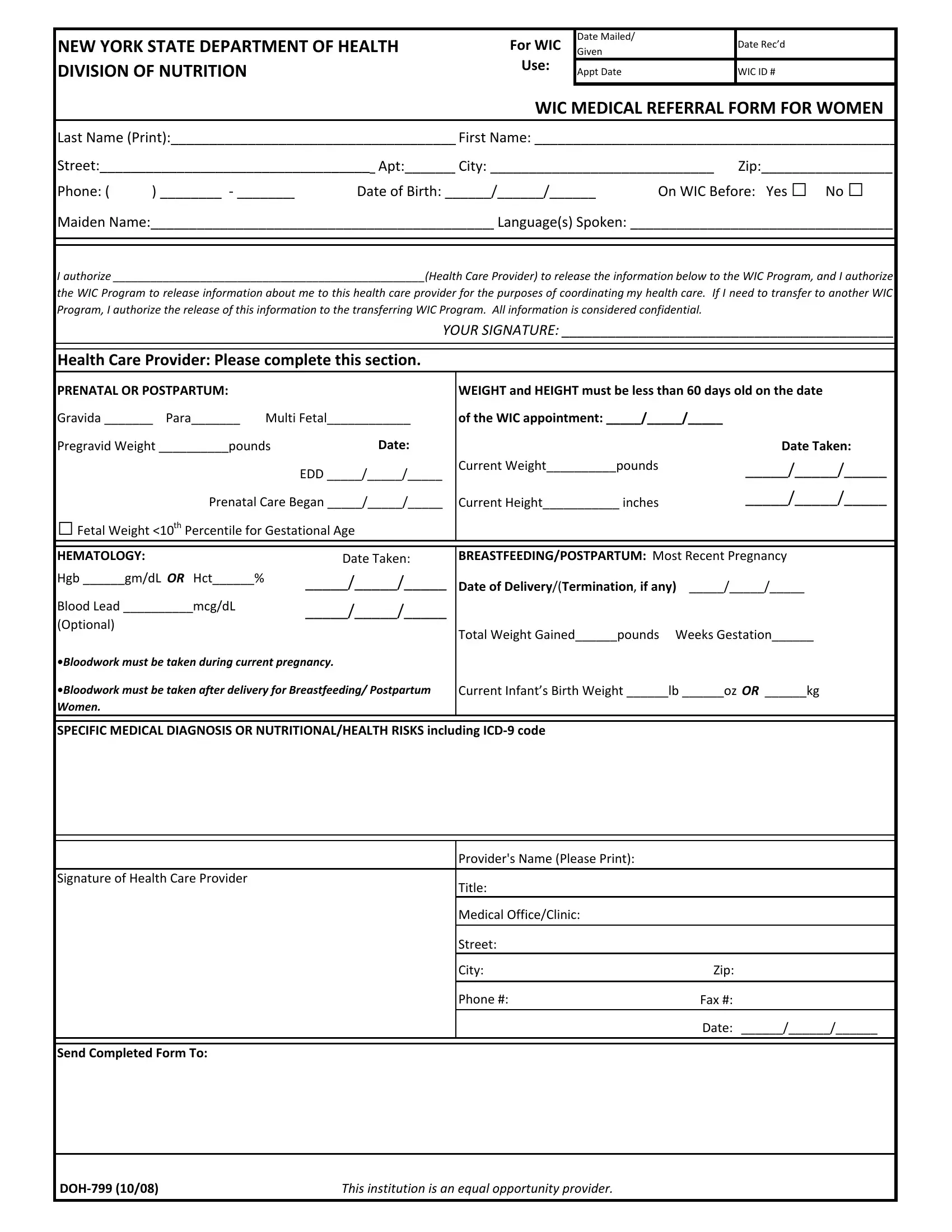
| Form Name | Medical Referral Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | printable wic forms ny state, wic form illinois pdf, medical referral form template, WIC |
Date Mailed/
Given
Date Rec’d
NEW YORK STATE DEPARTMENT OF HEALTH DIVISION OF NUTRITION
For WIC
Use:
Appt Date |
WIC ID # |
WIC MEDICAL REFERRAL FORM FOR WOMEN
Last Name (Print):_____________________________________ First Name: _______________________________________________
Street:____________________________________ Apt:_______ City: _____________________________ |
Zip:_________________ |
||||
Phone: ( |
) ________ ‐ ________ |
Date of Birth: ______/______/______ |
On WIC Before: Yes □ |
No □ |
|
Maiden Name:_____________________________________________ Language(s) Spoken: __________________________________
PRENATAL OR POSTPARTUM: |
|
|
WEIGHT and HEIGHT must be less than 60 days old on the date |
|
Gravida _______ Para_______ |
Multi Fetal____________ |
of the WIC appointment: _____/_____/_____ |
|
|
Pregravid Weight __________pounds |
Date: |
|
Date Taken: |
|
|
|
EDD _____/_____/_____ |
Current Weight__________pounds |
_____/_____/_____ |
|
|
|
||
Prenatal Care Began _____/_____/_____ |
Current Height___________ inches |
_____/_____/_____ |
||
□Fetal Weight <10th Percentile for Gestational Age
HEMATOLOGY: |
Date Taken: |
Hgb ______gm/dL OR Hct______% |
_____/_____/_____ |
Blood Lead __________mcg/dL |
_____/_____/_____ |
(Optional) |
|
•Bloodwork must be taken during current pregnancy.
•Bloodwork must be taken after delivery for Breastfeeding/ Postpartum Women.
BREASTFEEDING/POSTPARTUM: Most Recent Pregnancy
Date of Delivery/(Termination, if any) _____/_____/_____
Total Weight Gained______pounds Weeks Gestation______
Current Infant’s Birth Weight ______lb ______oz OR ______kg
SPECIFIC MEDICAL DIAGNOSIS OR NUTRITIONAL/HEALTH RISKS including ICD‐9 code
|
Provider's Name (Please Print): |
|
|
|
|
Signature of Health Care Provider |
Title: |
|
|
|
|
|
Medical Office/Clinic: |
|
|
|
|
|
Street: |
|
|
City: |
Zip: |
|
|
|
|
Phone #: |
Fax #: |
|
|
|
|
|
Date: ______/______/______ |
|
|
|
|
|
|
Send Completed Form To: |
|
|
DOH‐799 (10/08) |
This institution is an equal opportunity provider. |