It is straightforward to complete the claim reopening for medicare part b online empty lines. Our tool can make it nearly effortless to complete almost any PDF. Down below are the primary four steps you need to follow:
Step 1: Click the button "Get Form Here".
Step 2: Now, you're on the file editing page. You can add information, edit present details, highlight certain words or phrases, place crosses or checks, insert images, sign the template, erase unneeded fields, etc.
Feel free to enter the following details to prepare the claim reopening for medicare part b online PDF:
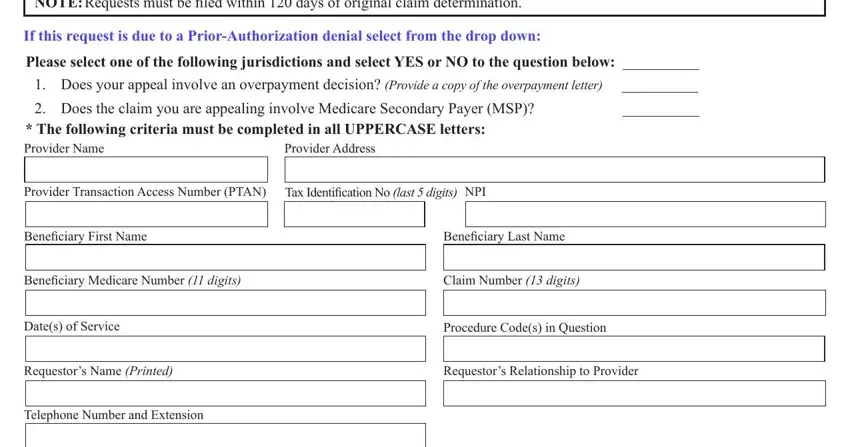
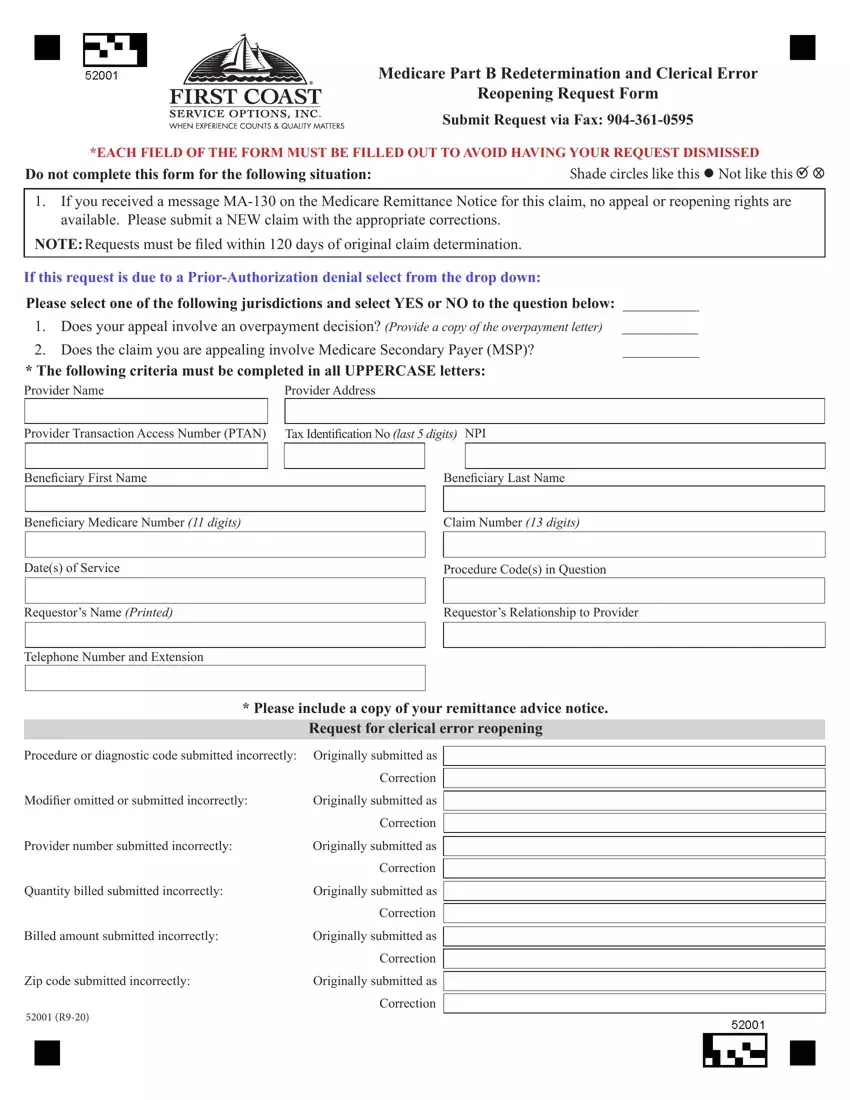
Put the required details in the Please include a copy of your, Procedure or diagnostic code, Modifier omitted or submitted, Originally submitted as, Correction, Correction, Provider number submitted, Originally submitted as, Correction, Quantity billed submitted, Originally submitted as, Correction, Billed amount submitted incorrectly, Originally submitted as, and Correction field.
You can be asked for some valuable information in order to fill in the The reason I disagree with the, This is an appeal of an, The service was medically necessary, The service was denied as a, The service was not overutilized, The service was denied indicating, Additional narrative, Please attach all pertinent, q Ambulance run sheet q Invoices, and q History and physical q field.
It is essential to indicate the rights and responsibilities of each side in space q Ambulance run sheet q Invoices, Improper use of this form and, Telephone reopenings can be, Unprocessable claims denied with, If the service at issue has, Appeals for durable medical, Overpayments resulting from, NOTICE Anyone who misrepresents, medicarefcsocom, Print, and Reset.
Step 3: Press the button "Done". The PDF form can be transferred. You will be able download it to your computer or send it by email.
Step 4: Be certain to remain away from possible worries by generating as much as a pair of copies of your form.
