The PDF editor was designed with the aim of allowing it to be as effortless and easy-to-use as it can be. The next steps are going to make creating the medication error reporting format simple.
Step 1: You should choose the orange "Get Form Now" button at the top of the webpage.
Step 2: Now you are going to be within the file edit page. It's possible to add, change, highlight, check, cross, include or remove areas or phrases.
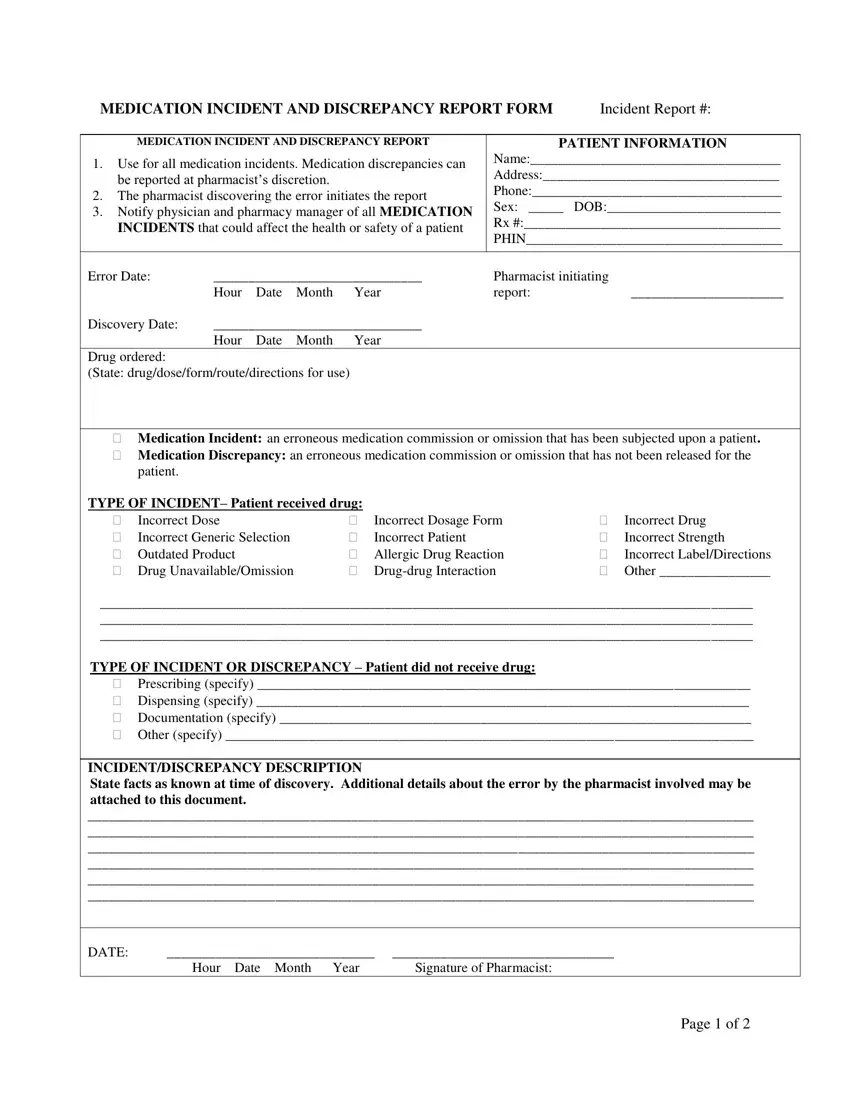
Enter the required data in every section to fill in the PDF medication error reporting format
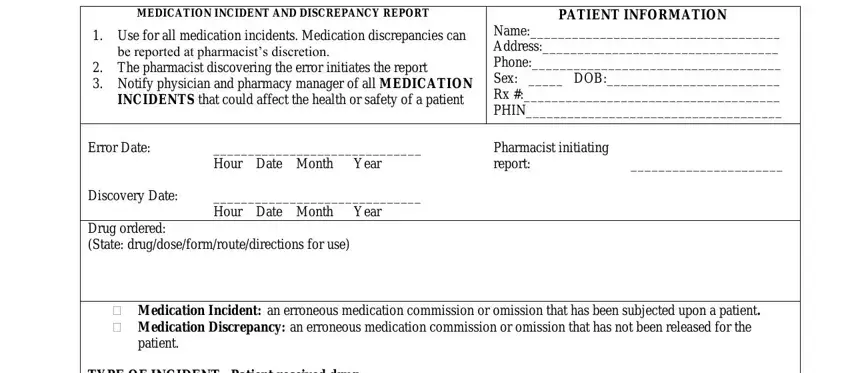
In the Incorrect Dose Incorrect Generic, TYPE OF INCIDENT Patient received, Outdated Product Drug, Incorrect Drug Incorrect, TYPE OF INCIDENT OR DISCREPANCY, Prescribing specify Dispensing, and INCIDENTDISCREPANCY DESCRIPTION area, note down your details.
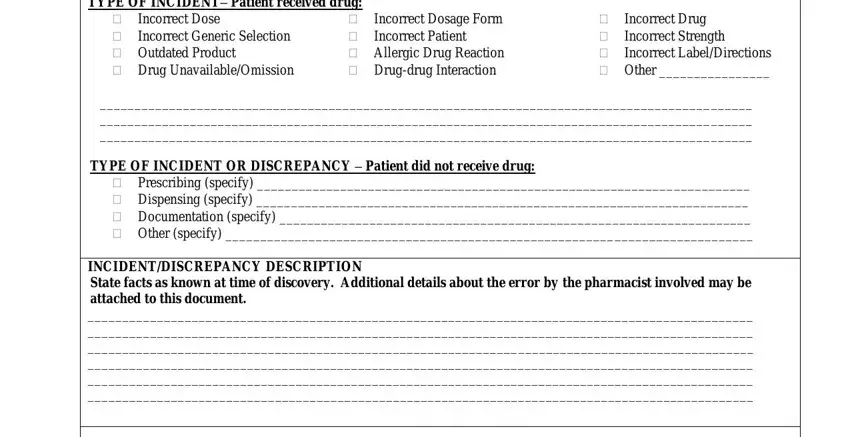
Within the segment discussing DATE Hour Date Month Year, Patient notified, Hour Date Month Year, Physician notified, YesNo, Hour Date Month Year, SEVERITY, None Minor Major, OUTCOME OF INVESTIGATION, No change in patients condition, required, Produces a temporary systemic or, not cause ongoing complications, and Requires immediate medical, you are required to type in some necessary details.
The Signature Date Pharmacist filling, Signature Date Pharmacy Manager, PHARMACY USE ONLY, and Page of box allows you to specify the rights and obligations of both sides.
Step 3: Choose the Done button to be sure that your finished file can be transferred to every gadget you prefer or sent to an email you indicate.
Step 4: You will need to generate as many copies of your form as you can to stay away from potential misunderstandings.
