Follow these steps to quickly complete the medication administration record in our PDF editor.
1. Complete the Header
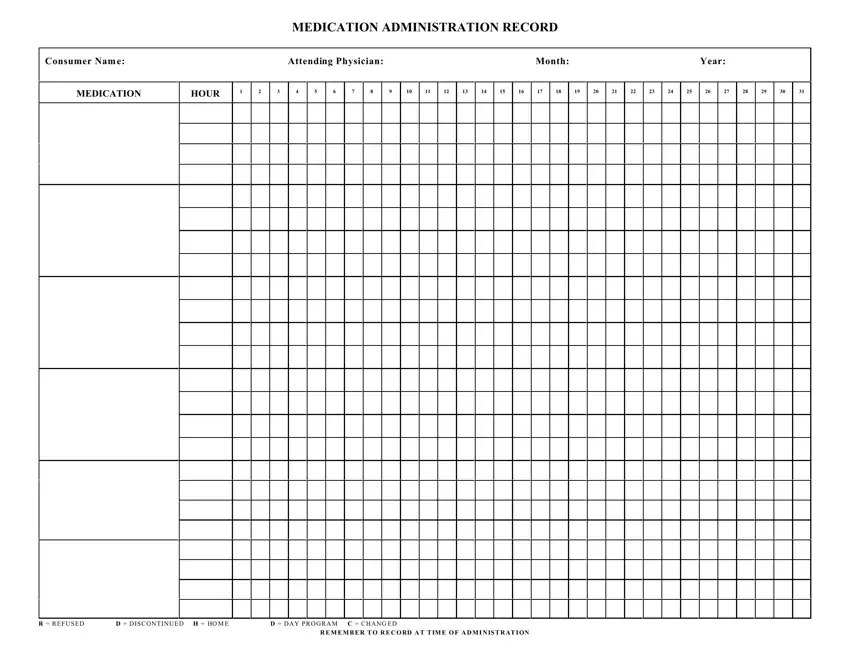
First, fill out the header section at the top of the medication administration record template. Write the consumer's and doctor's names, as well as the month and year the record covers.
2. List All Medications
Next, write each medication name in the left-hand Medication column. Use one row for each medication so the record stays clear and easy to follow.
If the person takes more than one medication, list them on separate lines instead of grouping them together.
Below is a MAR documentation example.
3. Daily Administration
Across the top of the form, the days of the month appear as numbered columns from 1 to 31. Each time you give a medication, mark the correct box for that day and hour.
Always write it down right away, rather than coming back to it later, to keep the record accurate.
4. Use Standard Abbreviations
You can use the approved MAR abbreviations on the form when needed:
- R - refused
- D - discontinued
- H - home
- D - day program
- C - changed
When the person does not take a scheduled dose, mark the appropriate letter instead of leaving the space blank.
Once you have finished, click the Done button in the editor. Then, you can save your PDF document to your device or send it via email.
5. Update When Needed
Continue updating the record daily throughout the month. If a medication changes or stops, reflect that change immediately on the form.
At the end of the month, review the record to confirm all entries are complete and legible.
