
Using PDF documents online is actually a breeze with this PDF editor. Anyone can fill out printable medical excuse forms here within minutes. Our tool is consistently developing to give the very best user experience possible, and that is thanks to our commitment to continual enhancement and listening closely to user feedback. All it takes is several basic steps:
Step 1: Just click the "Get Form Button" above on this webpage to start up our form editor. Here you will find everything that is needed to work with your document.
Step 2: This tool provides you with the ability to modify the majority of PDF files in many different ways. Change it with customized text, adjust what is originally in the file, and include a signature - all manageable within minutes!
Filling out this PDF requires thoroughness. Make sure all mandatory blank fields are filled out accurately.
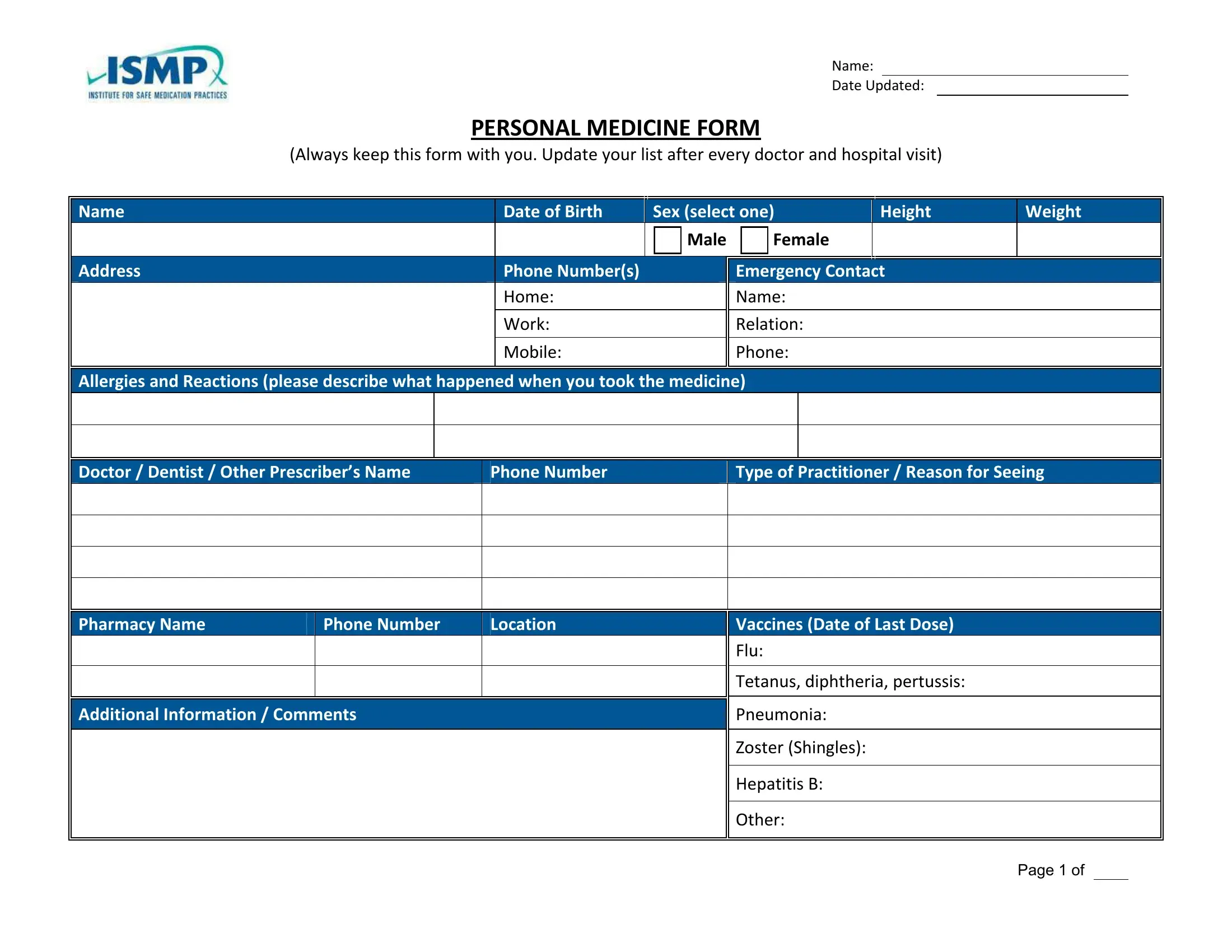
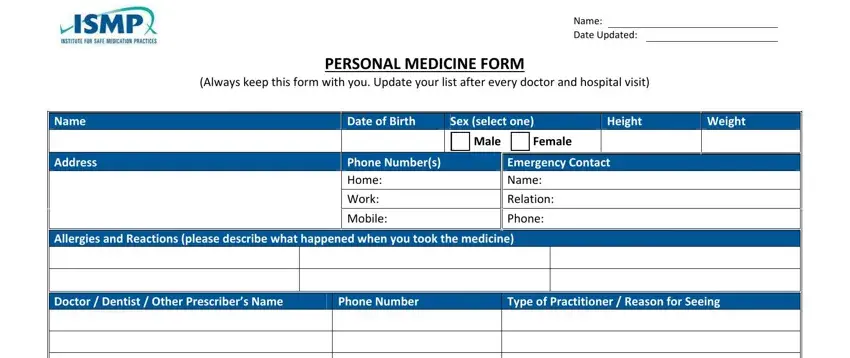
1. It's very important to fill out the printable medical excuse forms accurately, so be attentive while working with the areas containing these blanks:
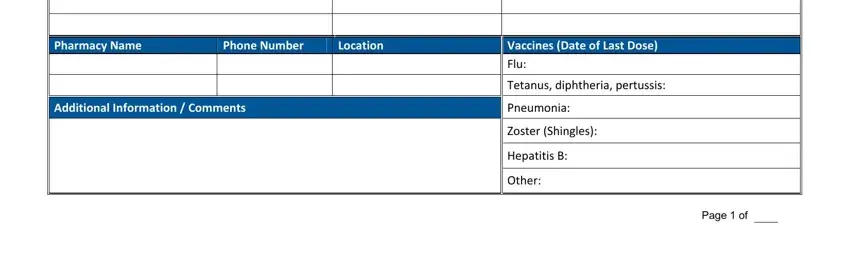
2. Once this part is done, it is time to include the needed specifics in Allergies and Reactions please, Phone Number Location, Phone Number, Type of Practitioner Reason for, Page of, Hepatitis B, and Other so you can move on further.
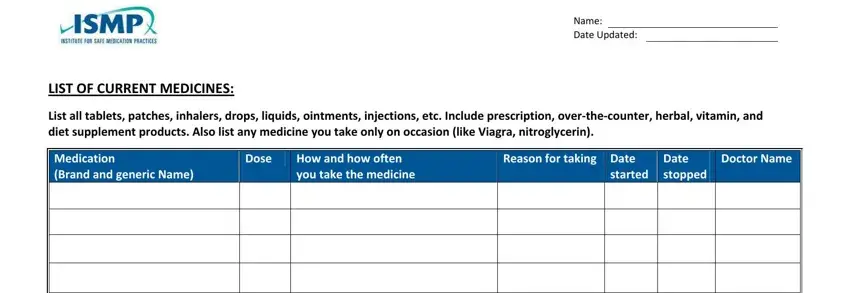
3. The following portion is about LIST OF CURRENT MEDICINES List all, Name Date Updated, Medication Brand and generic Name, Dose, How and how often you take the, Reason for taking Date, started, Date stopped, and Doctor Name - fill out each of these fields.
It is possible to make an error while filling out the LIST OF CURRENT MEDICINES List all, for that reason make sure you go through it again before you'll submit it.
4. The following section will require your input in the subsequent areas: Check here if additional pages are. Make certain to type in all requested info to go further.
5. Now, this last subsection is what you have to finish prior to using the PDF. The blank fields at issue are the next: Page of.

Step 3: Proofread everything you have typed into the blanks and click the "Done" button. Make a free trial option with us and gain instant access to printable medical excuse forms - with all adjustments saved and accessible inside your FormsPal account. FormsPal is devoted to the confidentiality of all our users; we make sure that all personal information going through our tool is kept confidential.