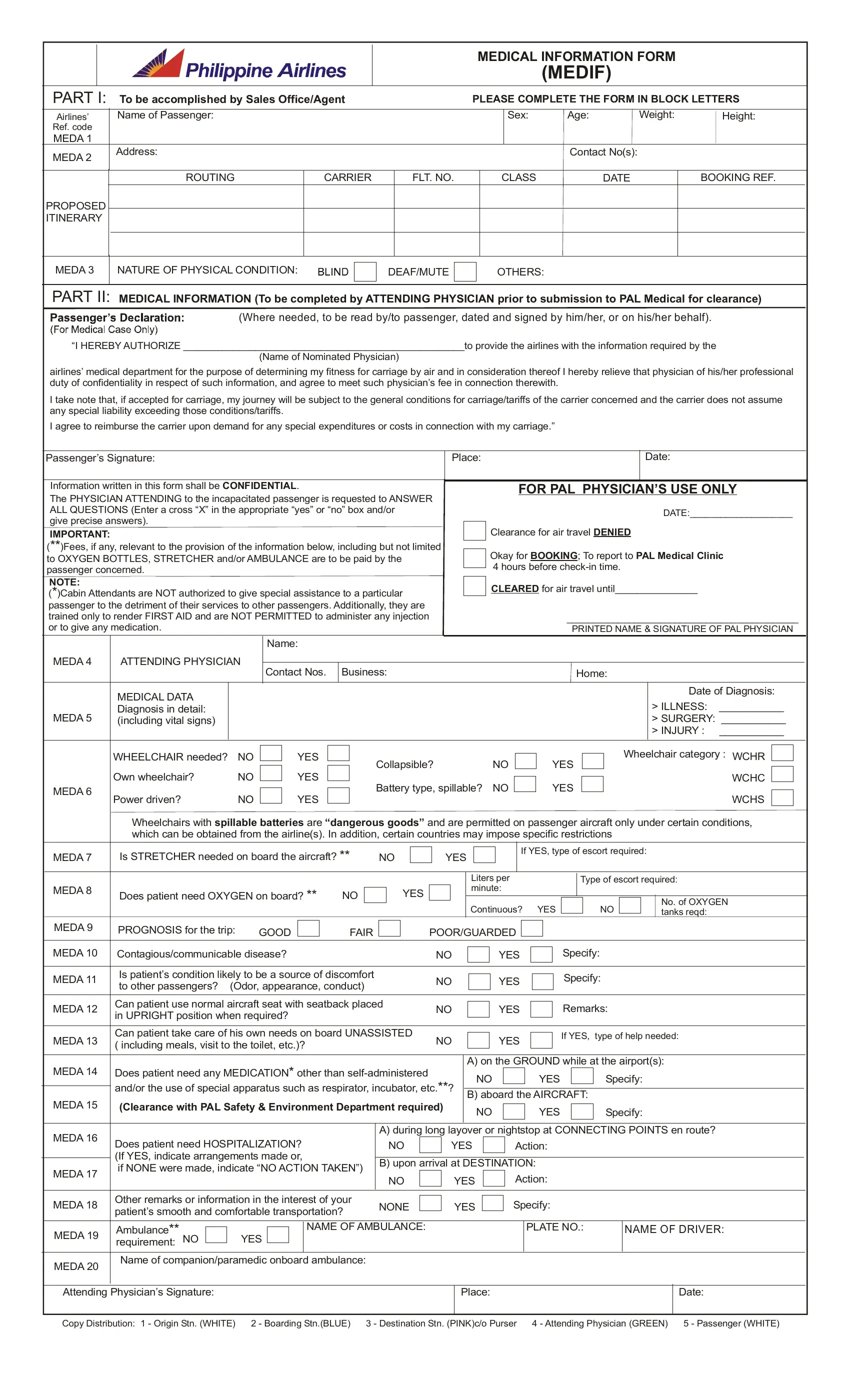
Traveling with certain medical conditions requires thorough preparation and clear communication with the airline, a fact underlined by the structure and content of the Medical Information Form (MEDIF) required by Qatar Airways. This form, an essential document, serves multiple purposes, including ensuring the safety of passengers with health issues during flights and facilitating necessary accommodations. The MEDIF form is divided into two main sections; the first part is completed by the sales office or booking agent, capturing basic passenger information and proposed itinerary details. The second, more critical part requires comprehensive medical information provided by the passenger's attending physician. This includes diagnosis, prognosis, and specific needs such as oxygen tanks, stretchers, or medication during the flight. Additionally, it confirms the passenger's ability to care for themselves or their requirement for special assistance. The completion of this form, which must be submitted prior to travel, activates a process within the airline to ensure all necessary preparations are in place, emphasizing the form's role not just in communication, but in passenger safety and comfort. Through stipulations regarding confidentiality and the relieving of the physician's duty of confidentiality, the form balances the need for medical transparency with respect for patient privacy. Furthermore, the conditional authorization for onboard and pre-flight medical requirements illustrates a comprehensive approach to passenger health. Ultimately, the MEDIF form showcases the airline's commitment to accommodating passengers with health considerations, ensuring they can travel with dignity and in safety.
| Question | Answer |
|---|---|
| Form Name | Medif Form Qatar Airways |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | qatar airways health form, qatar fit to fly, qatar airways medif form, qatar medical form |
|
|
|
|
|
|
|
MEDICAL INFORMATION FORM |
|
|
||||
|
|
|
|
|
|
|
|
|
|
(MEDIF) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
PART I: |
To be accomplished by Sales Office/Agent |
|
PLEASE COMPLETE THE FORM IN BLOCK LETTERS |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Airlines’ |
Name of Passenger: |
|
|
|
|
|
Sex: |
Age: |
Weight: |
Height: |
|||
Ref. code |
|
|
|
|
|
|
|
|
|
|
|
||
MEDA 1 |
|
|
|
|
|
|
|
|
|
|
|
||
MEDA 2 |
Address: |
|
|
|
|
|
|
Contact No(s): |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ROUTING |
CARRIER |
FLT. NO. |
|
CLASS |
DATE |
|
BOOKING REF. |
|
||
PROPOSED |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|||
ITINERARY |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDA 3
NATURE OF PHYSICAL CONDITION:
DEAF/MUTE
OTHERS:
PART II: MEDICAL INFORMATION (To be completed by ATTENDING PHYSICIAN prior to submission to PAL Medical for clearance)
(Where needed, to be read by/to passenger, dated and signed by him/her, or on his/her behalf).
“I HEREBY AUTHORIZE ___________________________________________________to provide the airlines with the information required by the
(Name of Nominated Physician)
airlines’ medical department for the purpose of determining my fitness for carriage by air and in consideration thereof I hereby relieve that physician of his/her professional duty of confidentiality in respect of such information, and agree to meet such physician’s fee in connection therewith.
I take note that, if accepted for carriage, my journey will be subject to the general conditions for carriage/tariffs of the carrier concerned and the carrier does not assume any special liability exceeding those conditions/tariffs.
I agree to reimburse the carrier upon demand for any special expenditures or costs in connection with my carriage.”
Passenger’s Signature:
Place:
Date:
|
Information written in this form shall be CONFIDENTIAL. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FOR PAL PHYSICIAN’S USE ONLY |
|
|||||||||||||||||||||||||||||||||
|
The PHYSICIAN ATTENDING to the incapacitated passenger is requested to ANSWER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
ALL QUESTIONS (Enter a cross “X” in the appropriate “yes” or “no” box and/or |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE:____________________ |
|
||||||||||||||||||||||||||||
|
give precise answers). |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Clearance for air travel DENIED |
|
|
|
|
||||||||||||||||||||||||||||
|
IMPORTANT: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
(**)Fees, if any, relevant to the provision of the information below, including but not limited |
|
|
|
|
|
Okay for BOOKING; To report to PAL Medical Clinic |
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
to OXYGEN BOTTLES, STRETCHER and/or AMBULANCE are to be paid by the |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
4 hours before |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||
|
passenger concerned. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
NOTE: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CLEARED for air travel until_______________ |
|
|
|
|
|||||||||||||||||||||||
|
(*)Cabin Attendants are NOT authorized to give special assistance to a particular |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
passenger to the detriment of their services to other passengers. Additionally, they are |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
trained only to render FIRST AID and are NOT PERMITTED to administer any injection |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_____________________________________________ |
|
|||||||||||||||||||||||||||||||||||||||
|
or to give any medication. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRINTED NAME & SIGNATURE OF PAL PHYSICIAN |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
MEDA 4 |
ATTENDING PHYSICIAN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Contact Nos. |
|
Business: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Home: |
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDICAL DATA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of Diagnosis: |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
MEDA 5 |
Diagnosis in detail: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
> ILLNESS: |
___________ |
|
|
|||
|
(including vital signs) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
> SURGERY: ___________ |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
> INJURY : |
___________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Wheelchair category : WCHR |
|
|
|
||||
|
|
WHEELCHAIR needed? |
NO |
|
|
|
|
|
YES |
|
|
|
|
Collapsible? |
|
|
|
|
|
|
|
|
|
NO |
|
|
|
|
|
|
YES |
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
Own wheelchair? |
NO |
|
|
|
|
|
YES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
WCHC |
|
|
|
|||||||||||||||||||||||
|
MEDA 6 |
|
|
|
|
|
|
|
|
|
Battery type, spillable? |
NO |
|
|
|
|
|
|
|
YES |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
Power driven? |
NO |
|
|
|
|
|
YES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
WCHS |
|
|
|
|||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Wheelchairs with spillable batteries are “dangerous goods” and are permitted on passenger aircraft only under certain conditions, |
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
which can be obtained from the airline(s). In addition, certain countries may impose specific restrictions |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDA 7 |
Is STRETCHER needed on board the aircraft? ** |
|
NO |
|
|
|
|
|
YES |
|
|
|
|
|
|
|
|
|
If YES, type of escort required: |
|
|
|
|
||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Liters per |
|
|
|
|
|
|
|
Type of escort required: |
|
|
|
|
|||||||||||||||||||
|
MEDA 8 |
Does patient need OXYGEN on board? ** |
|
NO |
|
|
|
|
YES |
|
|
|
|
|
|
minute: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Continuous? |
|
|
YES |
|
|
|
|
|
|
NO |
|
|
|
No. of OXYGEN |
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
tanks reqd: |
|
|
|
|
||||||||||||||||
|
MEDA 9 |
PROGNOSIS for the trip: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
GOOD |
|
|
|
|
|
FAIR |
|
|
|
|
|
|
POOR/GUARDED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDA 10 |
Contagious/communicable disease? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NO |
|
|
|
|
|
|
|
YES |
|
|
|
|
|
Specify: |
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDA 11 |
Is patient’s condition likely to be a source of discomfort |
|
|
|
|
|
|
|
|
NO |
|
|
|
|
|
|
|
YES |
|
|
|
|
|
Specify: |
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
to other passengers? (Odor, appearance, conduct) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
MEDA 12 |
Can patient use normal aircraft seat with seatback placed |
NO |
|
|
|
|
|
|
|
YES |
|
|
|
|
|
Remarks: |
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||
|
in UPRIGHT position when required? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
MEDA 13 |
Can patient take care of his own needs on board UNASSISTED |
NO |
|
|
|
|
|
|
|
YES |
|
|
|
|
|
If YES, type of help needed: |
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||
|
( including meals, visit to the toilet, etc.)? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
Does patient need any MEDICATION* other than |
|
|
|
|
A) on the GROUND while at the airport(s): |
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||
|
MEDA 14 |
|
|
|
|
|
NO |
|
|
|
|
|
|
|
|
YES |
|
|
|
|
|
|
|
Specify: |
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
and/or the use of special apparatus such as respirator, incubator, etc.**? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||
|
|
B) aboard the AIRCRAFT: |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
MEDA 15 |
(Clearance with PAL Safety & Environment Department required) |
|
|
NO |
|
|
|
|
|
|
|
|
YES |
|
|
|
|
|
|
|
Specify: |
|
|
|
|
||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDA 16 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A) during long layover or nightstop at CONNECTING POINTS en route? |
|
|
|
|
||||||||||||||||||||||||||||||||||||||
|
Does patient need HOSPITALIZATION? |
|
|
|
|
|
|
NO |
|
|
|
|
|
YES |
|
|
|
|
|
|
|
Action: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
(If YES, indicate arrangements made or, |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
B) upon arrival at DESTINATION: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||
|
|
if NONE were made, indicate “NO ACTION TAKEN”) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||
|
MEDA 17 |
|
|
NO |
|
|
|
|
|
|
YES |
|
|
|
|
|
|
|
Action: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDA 18 |
Other remarks or information in the interest of your |
|
NONE |
|
|
|
|
|
|
YES |
|
|
|
|
|
Specify: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
patient’s smooth and comfortable transportation? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
MEDA 19 |
Ambulance** |
|
|
|
|
|
|
|
|
|
|
NAME OF AMBULANCE: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PLATE NO.: |
NAME OF DRIVER: |
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||
|
requirement: NO |
|
|
|
YES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
MEDA 20 |
Name of companion/paramedic onboard ambulance: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Attending Physician’s Signature:
Place:
Date:
Copy Distribution: 1 - Origin Stn. (WHITE) |
2 - Boarding Stn.(BLUE) 3 - Destination Stn. (PINK)c/o Purser 4 - Attending Physician (GREEN) |
5 - Passenger (WHITE) |