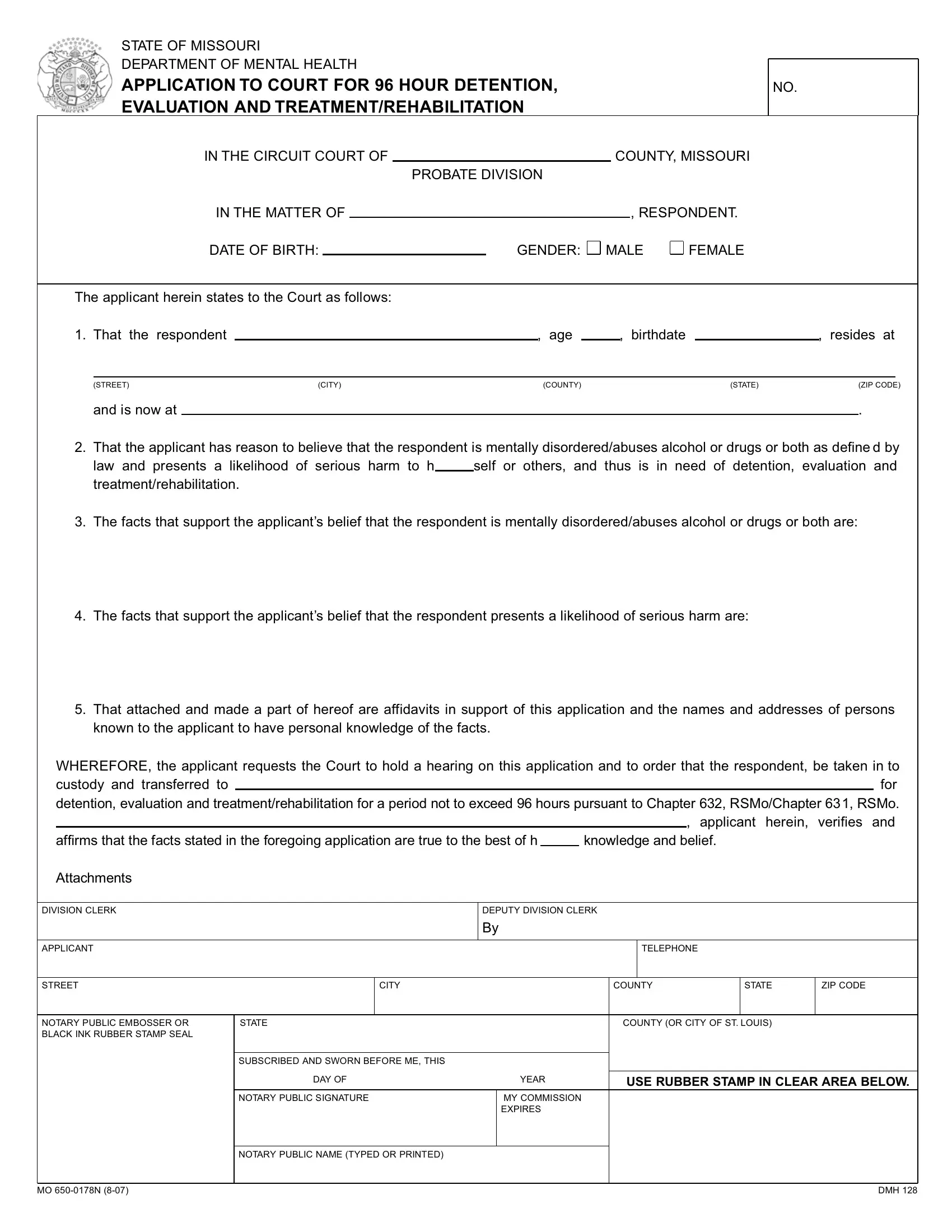
At the heart of addressing mental health crises within the community, the state of Missouri employs a comprehensive approach through the use of a specific legal instrument, the Mental Health Form. This document serves as an application to the court for the 96-hour detention, evaluation, and treatment or rehabilitation of individuals believed to be in a state of mental disorder or substance abuse that poses a serious risk to themselves or others. The procedural aspect involves an applicant, who claims to have reasonable grounds, providing detailed information about the respondent, including residence and personal details, alongside a narrative on the perceived mental health or substance abuse issues and the associated risks. Critical to this process are affidavits and contact details of witnesses supporting the application, which underline the importance of corroborative evidence in these sensitive situations. The ultimate goal, as facilitated by this form, is to ensure a swift judicial review that could authorize the short-term detention of the respondent in a specialized facility for the necessary medical evaluation and possible intervention. This legal tool underscores a broader commitment to public safety and health, balancing individual rights with community welfare within Missouri's judicial framework.
| Question | Answer |
|---|---|
| Form Name | Mental Health Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | missouri 96 hour detention, mo 96 hour, missouri form 96 hour, 96 hour hold |
STATE OF MISSOURI
DEPARTMENT OF MENTAL HEALTH
APPLICATION TO COURT FOR 96 HOUR DETENTION, EVALUATION AND TREATMENT/REHABILITATION
NO.
IN THE CIRCUIT COURT OF |
|
|
COUNTY, MISSOURI |
||||
|
|
|
PROBATE DIVISION |
|
|||
IN THE MATTER OF |
|
|
|
|
, RESPONDENT. |
||
DATE OF BIRTH: |
|
|
GENDER: MALE |
FEMALE |
|||
The applicant herein states to the Court as follows:
1. That the |
respondent |
|
, age |
|
, birthdate |
|
, |
resides at |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(STREET) |
|
|
(CITY) |
(COUNTY) |
|
|
(STATE) |
|
(ZIP CODE) |
||
|
and is now at |
|
|
|
|
|
|
|
. |
|
||
2.That the applicant has reason to believe that the respondent is mentally disordered/abuses alcohol or drugs or both as define d by
law and presents a likelihood of serious harm to h self or others, and thus is in need of detention, evaluation and treatment/rehabilitation.
3.The facts that support the applicant’s belief that the respondent is mentally disordered/abuses alcohol or drugs or both are:
4.The facts that support the applicant’s belief that the respondent presents a likelihood of serious harm are:
5.That attached and made a part of hereof are affidavits in support of this application and the names and addresses of persons known to the applicant to have personal knowledge of the facts.
WHEREFORE, the applicant requests the Court to hold a hearing on this application and to order that the respondent, be taken in to
custody and transferred tofor
detention, evaluation and treatment/rehabilitation for a period not to exceed 96 hours pursuant to Chapter 632, RSMo/Chapter 631, RSMo.
|
|
|
|
|
|
|
|
|
|
|
, applicant herein, verifies and |
||
|
affirms that the facts stated in the foregoing application are true to the best of h |
|
|
knowledge and belief. |
|
|
|||||||
|
Attachments |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DIVISION CLERK |
|
|
DEPUTY DIVISION CLERK |
|
|
||||||||
|
|
|
|
By |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
APPLICANT |
|
|
|
|
|
|
|
|
TELEPHONE |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STREET |
|
CITY |
|
|
|
|
|
COUNTY |
STATE |
ZIP CODE |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NOTARY PUBLIC EMBOSSER OR |
STATE |
|
|
|
|
|
COUNTY (OR CITY OF ST. LOUIS) |
|
|||||
BLACK INK RUBBER STAMP SEAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SUBSCRIBED AND SWORN BEFORE ME, THIS |
|
|
|
|
|
|
|
|
|
|
|
|
|
DAY OF |
|
YEAR |
|
|
|
|
|
|
|||
|
|
|
|
USE RUBBER STAMP IN CLEAR AREA BELOW. |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NOTARY PUBLIC SIGNATURE |
|
MY COMMISSION |
|
|
|
|
|
|
|||
|
|
|
|
|
EXPIRES |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NOTARY PUBLIC NAME (TYPED OR PRINTED) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MO |
DMH 128 |