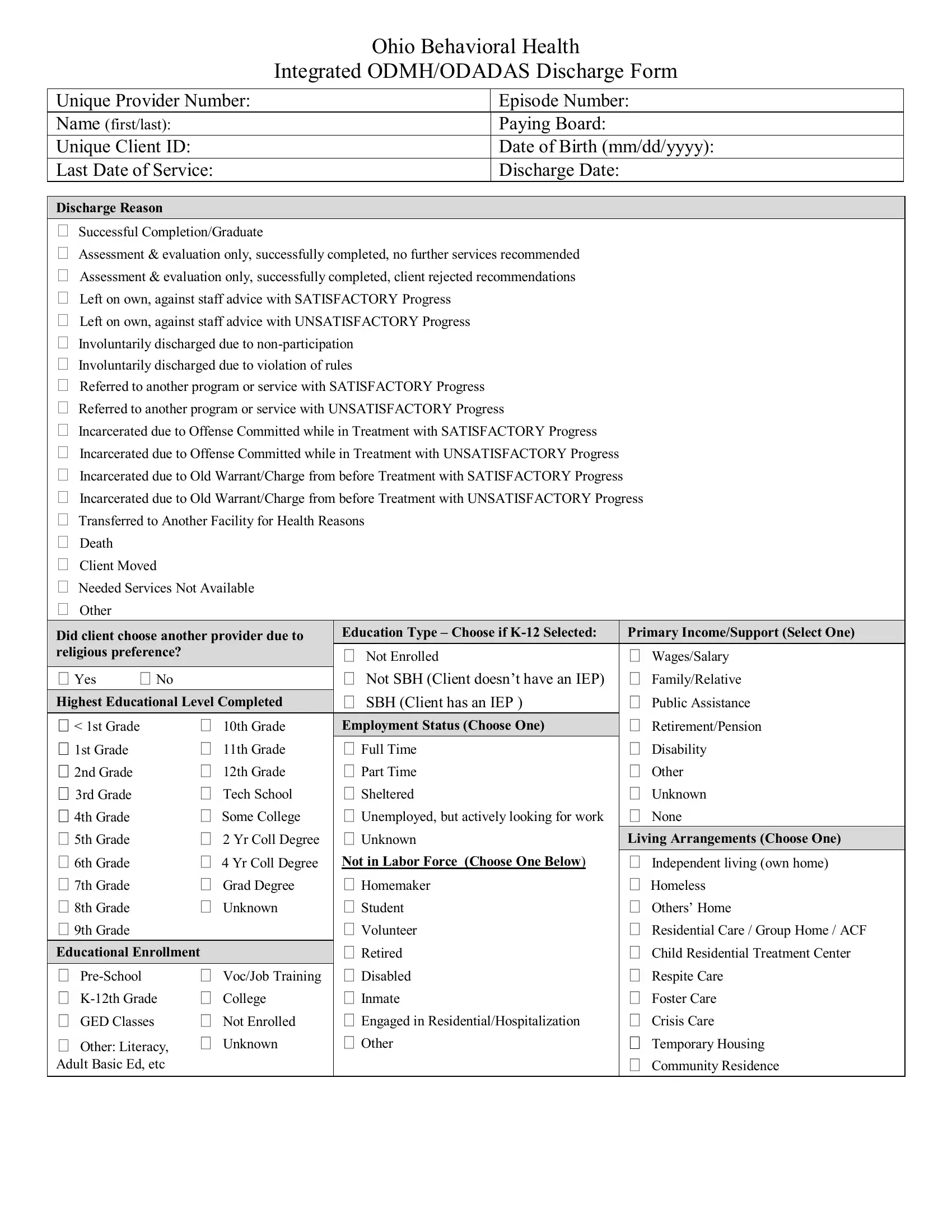
In Ohio, the Behavioral Discharge form is a comprehensive document used by behavioral health providers to encapsulate a client's journey through treatment, including their progress and the outcome at discharge. This form captures a wide array of information, including the provider's unique number, episode number, client's personal details (such as name, date of birth, and unique client ID), and financial details like the paying board. It marks the last date of service alongside the discharge date, providing clear reasons for discharge that range from successful completion to involuntary discharge due to non-participation or violation of rules. Various outcomes, including referral to another program or incarceration due to offenses committed while in treatment, can be noted with distinctions made based on the client's progress. This form further collects data on education, primary income, living arrangements, drug of choice, health conditions, and diagnoses, offering a multifaceted view of the client’s situation. Importantly, it includes the client's self-reported physical health conditions, such as diabetes or cardiovascular disease, which can have significant implications for treatment and aftercare. Also of note are sections detailing the client's engagement with evidence-based practices, self-help program attendance towards discharge, and whether the client uses tobacco products, providing a holistic overview of the client’s treatment episode and readiness for discharge. This form serves as a critical tool for ensuring continuity of care and supporting the ongoing recovery of individuals transitioning out of behavioral health services.
| Question | Answer |
|---|---|
| Form Name | Ohio Behavioral Discharge Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | discharge form ohio behavioral health discharge form |
|
Ohio Behavioral Health |
|
|
Integrated ODMH/ODADAS Discharge Form |
|
|
|
|
Unique Provider Number: |
|
Episode Number: |
Name (first/last): |
|
Paying Board: |
Unique Client ID: |
|
Date of Birth (mm/dd/yyyy): |
Last Date of Service: |
|
Discharge Date: |
Discharge Reason
Successful Completion/Graduate
Assessment & evaluation only, successfully completed, no further services recommended
Assessment & evaluation only, successfully completed, client rejected recommendations
Left on own, against staff advice with SATISFACTORY Progress
Left on own, against staff advice with UNSATISFACTORY Progress
Involuntarily discharged due to
Involuntarily discharged due to violation of rules
Referred to another program or service with SATISFACTORY Progress
Referred to another program or service with UNSATISFACTORY Progress
Incarcerated due to Offense Committed while in Treatment with SATISFACTORY Progress
Incarcerated due to Offense Committed while in Treatment with UNSATISFACTORY Progress
Incarcerated due to Old Warrant/Charge from before Treatment with SATISFACTORY Progress
Incarcerated due to Old Warrant/Charge from before Treatment with UNSATISFACTORY Progress
Transferred to Another Facility for Health Reasons
Death
Client Moved
Needed Services Not Available
Other
|
|
|
|
|
|
Education Type – Choose if |
|
|
Primary Income/Support (Select One) |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
||||||||
|
Did client choose another provider due to |
|
||||||||
|
religious preference? |
|
|
|
Not Enrolled |
|
Wages/Salary |
|||
|
|
|
|
|
|
|
||||
|
Yes |
No |
|
|
|
Not SBH (Client doesn’t have an IEP) |
|
Family/Relative |
||
|
Highest Educational Level Completed |
|
|
SBH (Client has an IEP ) |
|
Public Assistance |
||||
|
|
|
|
|||||||
|
< 1st Grade |
|
10th Grade |
|
Employment Status (Choose One) |
|
|
Retirement/Pension |
||
|
1st Grade |
|
11th Grade |
|
Full Time |
|
Disability |
|||
|
2nd Grade |
|
12th Grade |
|
Part Time |
|
Other |
|||
|
3rd Grade |
|
Tech School |
|
Sheltered |
|
Unknown |
|||
|
4th Grade |
|
Some College |
|
Unemployed, but actively looking for work |
|
None |
|||
|
5th Grade |
|
2 Yr Coll Degree |
|
Unknown |
|
Living Arrangements (Choose One) |
|
||
|
6th Grade |
|
4 Yr Coll Degree |
|
Not in Labor Force (Choose One Below) |
|
Independent living (own home) |
|||
|
7th Grade |
|
Grad Degree |
|
Homemaker |
|
Homeless |
|||
|
8th Grade |
|
Unknown |
|
Student |
|
Others’ Home |
|||
|
9th Grade |
|
|
|
|
Volunteer |
|
Residential Care / Group Home / ACF |
||
|
|
|
|
Retired |
|
Child Residential Treatment Center |
||||
|
Educational Enrollment |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Voc/Job Training |
|
Disabled |
|
Respite Care |
||||
|
College |
|
Inmate |
|
Foster Care |
|||||
|
GED Classes |
|
Not Enrolled |
|
Engaged in Residential/Hospitalization |
|
Crisis Care |
|||
|
Other: Literacy, |
Unknown |
|
Other |
|
Temporary Housing |
||||
Adult Basic Ed, etc |
|
|
|
|
|
|
Community Residence |
|||
|
|
|
|
|
|
|
|
|
|
|
|
Living Arrangements (continued) |
|
|
Drug of Choice (Continued) |
|
|
ODMH: BIOMARKERS |
|
|||||||
|
|
|
|
|
|
||||||||||
|
Nursing Facility |
|
|
|
|
|
|
|
|||||||
|
|
|
|
Source of Height/Weight Information |
|
||||||||||
|
Licensed MR Facility |
|
|
Other Opiates and Synthetics |
|
||||||||||
|
State MH/MR Institution |
|
|
PCP |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Hospital |
|
|
|
Other Hallucinogens |
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
Height and Weight |
|
|||||||
|
Correctional Facility |
|
|
Methamphetamines |
|
|
|
|
|
Height (feet and inches) |
|||||
|
Other |
|
|
|
Other Amphetamines |
|
|
| |
|
||||||
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|||||||
|
Unknown |
|
|
Other Stimulants |
|
|
|
|
|
Weight (lbs) |
|||||
|
|
|
|
|
|
Benzodiazepines |
|
|
| |
|
|||||
|
|
|
Global Assessment of |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
||||||
| |
|
Functioning |
|
|
Other |
|
Physical Health Conditions |
|
|||||||
|
Diagnosis Type (Choose One) |
|
|
Barbiturates |
|
|
|
Does client report/provide evidence of any of the |
|||||||
|
DSM IV |
ICD9 |
|
|
Other |
|
following conditions in past year? |
||||||||
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
Diabetes |
|
|
|||||
|
Primary Diagnosis Code: |
|
|
Inhalants |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
High Cholesterol |
||||||||
|
|
|
|
|
|
Nicotine |
|
|
|
|
Cardiovascular Disease (heart attack, stroke) |
||||
|
Secondary Diagnosis Code: |
|
|
Other Medications |
|
|
|
High blood pressure |
|||||||
|
|
|
|
|
|
Unknown |
|
|
|
Cancer |
|
|
|||
|
|
|
|
|
|
Frequency of Use |
|
|
|
Kidney Disease/Failure |
|||||
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
– 3 X Past Week |
|
Bowel Obstruction (eg, constipation) |
|||||||
|
Tertiary Diagnosis Code: |
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
– 2 X in Past Mo |
– 6 X Past Week |
|
Respiratory Disease (eg, COPD) |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
None |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Special Populations (Select all that Apply) |
|
|
Route of Administration |
|
|
|
Health Care Utilization |
|
||||||
|
SMD/SED |
|
|
Oral |
|
Injection |
|
How frequently (in days) has the client used the |
|||||||
|
Alcohol/Other Drug Abuse |
|
|
Smoking |
|
Other |
|
following since admission or last update? |
|||||||
|
|
|
|
|
|
|
|
|
|||||||
|
Forensic Status |
|
|
Inhalation |
Unknown |
|
|
|
|
|
|||||
|
|
|
|
|
|
Hospital Admissions |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
| |
|
|||
|
Developmentally Disabled |
|
|
|
|
Age of First Use – First |
|
||||||||
|
|
|
|
|
|
|
|
||||||||
|
Deaf/Hard of Hearing |
|
| |
|
Intoxication |
|
|
|
|
|
Emergency Room Visits/Admits |
||||
|
|
|
|
|
|
|
|
|
|||||||
|
Blind/Sight Impaired |
|
|
Primary AOD Code: |
|
|
| |
|
(psychiatric or physical health) |
||||||
|
|
|
|
|
|
|
|
||||||||
|
Physically Disabled |
|
|
|
|
Number of Arrests past 30 days |
|
|
|
Outpatient Primary Care Visits |
|||||
|
Sexual Abuse Victim |
|
| |
|
(AOD NOM) |
| |
|
(physical health) |
|||||||
|
Domestic Violence Victim/Witness |
|
|
Primary Reimbursement (Select One) |
|
|
|
|
Dental Visits |
||||||
|
Child of Alcohol/Drug Abuser |
|
|
|
|
|
|
| |
|
||||||
|
|
|
|
|
|
|
|
|
|||||||
|
HIV/AIDS |
|
|
Blue Cross/Blue Shield |
|
|
|
Evidence Based Practices |
|
||||||
|
Suicidal |
|
|
|
Medicare |
|
|
|
|
Did the client receive any of the following EBPs |
|||||
|
Language Barriers/English 2ND Lang. |
|
|
Medicaid |
|
|
|
|
since admission or last update? |
||||||
|
Hepatitis C |
|
|
Other Government Support |
|
Adult Practices |
|
||||||||
|
Transgendered |
|
|
Worker’s Compensation |
|
Supportive Housing |
|||||||||
|
In Custody/Child Welfare |
|
|
Other Private Health Insurance |
|
Supported Employment |
|||||||||
|
Multiple Service System Involvement |
|
|
No Charge |
|
|
|
Assertive Community Treatment (ACT) |
|||||||
|
|
|
|
Other Payment Source |
|
|
|
|
|
||||||
|
Early Childhood: At Risk for SED |
|
|
|
|
|
Family |
|
|||||||
|
Sexual Offender |
|
|
|
|
IDDT |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
Frequency of attendance at |
|
|
|
|
||||||||
|
Bisexual/Gay/Lesbian |
|
|
programs in the 30 days prior to discharge |
|
|
WMR/Illness |
||||||||
|
|
|
|
|
|
|
|
|
|||||||
|
Military Family |
|
|
No attendance in past month |
|
Medication Management |
|||||||||
|
Drug of Choice (Primary Choice) |
|
|
|
Child & Adolescent Practices |
|
|||||||||
|
Alcohol |
|
|
|
|
Therapeutic Foster Care |
|||||||||
|
Cocaine/Crack |
|
|
Some but unknown |
Unknown |
|
|
||||||||
|
|
|
|
|
|
Functional Family Therapy |
|||||||||
|
Marijuana/Hashish |
|
|
Does the client use tobacco products? |
|
|
|||||||||
|
Heroin |
|
|
|
Yes |
No |
Don’t Know |
|
Intensive |
||||||
|
Drug of Choice (Secondary) |
|
|
Drug of Choice (Tertiary) |
|
|
||||
|
|
|
|
|
||||||
|
Alcohol |
|
|
|
Alcohol |
|
|
|
||
|
Cocaine/Crack |
|
|
Cocaine/Crack |
|
|||||
|
Marijuana/Hashish |
|
|
Marijuana/Hashish |
|
|||||
|
Heroin |
|
|
|
Heroin |
|
|
|
||
|
|
|||||||||
|
Other Opiates and Synthetics |
|
Other Opiates and Synthetics |
|||||||
|
PCP |
|
|
|
PCP |
|
|
|
||
|
Other Hallucinogens |
|
|
Other Hallucinogens |
|
|||||
|
Methamphetamines |
|
|
Methamphetamines |
|
|||||
|
Other Amphetamines |
|
|
Other Amphetamines |
|
|||||
|
Other Stimulants |
|
|
Other Stimulants |
|
|||||
|
Benzodiazepines |
|
|
Benzodiazepines |
|
|||||
|
Other |
|
Other |
|||||||
|
Barbiturates |
|
|
Barbiturates |
|
|||||
|
Other |
|
Other |
|||||||
|
Inhalants |
|
|
|
Inhalants |
|
|
|
||
|
|
|||||||||
|
Nicotine |
|
|
|
Nicotine |
|
|
|
||
|
Other Medications |
|
|
Other Medications |
|
|||||
|
Unknown |
|
|
Unknown |
|
|||||
|
None |
|
|
|
None |
|
|
|
||
Frequency of Use |
|
Frequency of Use |
|
|||||||
|
No use Past Mo |
1 – 3 X Past Week |
|
No use Past Mo |
1 – 3 X Past Week |
|||||
|
1 – 2 X in Past Mo |
3 – 6 X Past Week |
|
1 – 2 X in Past Mo |
3 – 6 X Past Week |
|||||
|
Daily |
|
Unknown |
|
Daily |
|
|
Unknown |
||
Route of Administration |
|
Route of Administration |
|
|||||||
|
Oral |
|
Injection |
|
Oral |
|
|
Injection |
||
|
Smoking |
|
Other |
|
Smoking |
|
|
Other |
||
|
Inhalation |
|
Unknown |
|
Inhalation |
|
|
Unknown |
||
|
|
|
|
|
|
|
|
|||
|
|
|
Age of First Use – First |
|
|
|
Age of First Use – First |
|||
| |
|
Intoxication |
|
| |
|
Intoxication |
|
|||
|
|
|
|
|
|
|
||||
|
Secondary AOD Code |
|
|
Tertiary AOD Code |
|
|||||
|
|
|
|
|
|
|
|
|
|
|