

It is possible to fill out merck instantly with the help of our online tool for PDF editing. The editor is constantly maintained by our team, acquiring cool functions and becoming better. Getting underway is easy! Everything you need to do is take the following basic steps down below:
Step 1: First of all, open the pdf editor by clicking the "Get Form Button" above on this page.
Step 2: Once you start the file editor, you will get the form all set to be filled out. Besides filling in different fields, you can also do other actions with the file, particularly adding custom textual content, changing the original text, inserting images, affixing your signature to the form, and more.
For you to complete this form, ensure you type in the information you need in every single field:
1. To start with, when filling in the merck, begin with the page that has the next blank fields:
2. Once your current task is complete, take the next step – fill out all of these fields - Applicant Declarations and, SIGN, Patients Original Signature Date, M M, Applicant Authorization for Use, SIGN, Patients Original Signature Date, M M, You do not have to be a US citizen, Physician must complete Sections, and Merckhelpscom with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. Completing THIS IS THE PRESCRIPTION PLEASE DO, Patients First Name, Last Name, Date of Birth, Product Name, Product Name, Product Name, M M, Strength, Quantity, Directions, Refill, or Times, Strength, and Quantity is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
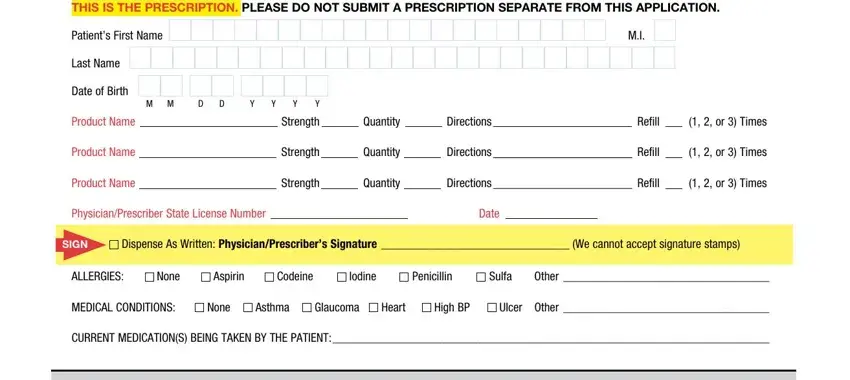
It is easy to get it wrong while filling out your Product Name, therefore ensure that you go through it again before you finalize the form.
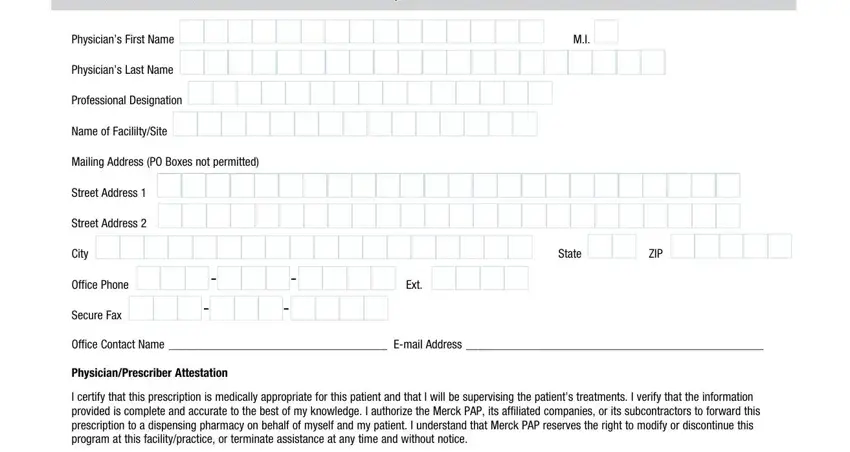
4. Now fill out this next segment! In this case you will get all of these SECTION PHYSICIANPRESCRIBER MUST, Physicians First Name, Physicians Last Name, Professional Designation, Name of FacililtySite, Mailing Address PO Boxes not, Street Address, Street Address, City, Office Phone, Secure Fax, Ext, State, ZIP, and Office Contact Name Email Address blanks to fill in.
5. Because you come close to the finalization of your file, there are a few more requirements that need to be satisfied. Mainly, SIGN, PhysiciansPrescribers Original, Date, M M, This form should not be tampered, To report an adverse event to a, CORP, Tear here place enrollment form in, and Merckhelpscom must all be filled out.
Step 3: After taking another look at your fields and details, click "Done" and you're all set! Right after creating afree trial account here, you will be able to download merck or email it right off. The PDF form will also be readily accessible via your personal cabinet with your changes. FormsPal is dedicated to the confidentiality of our users; we make certain that all information coming through our tool stays confidential.