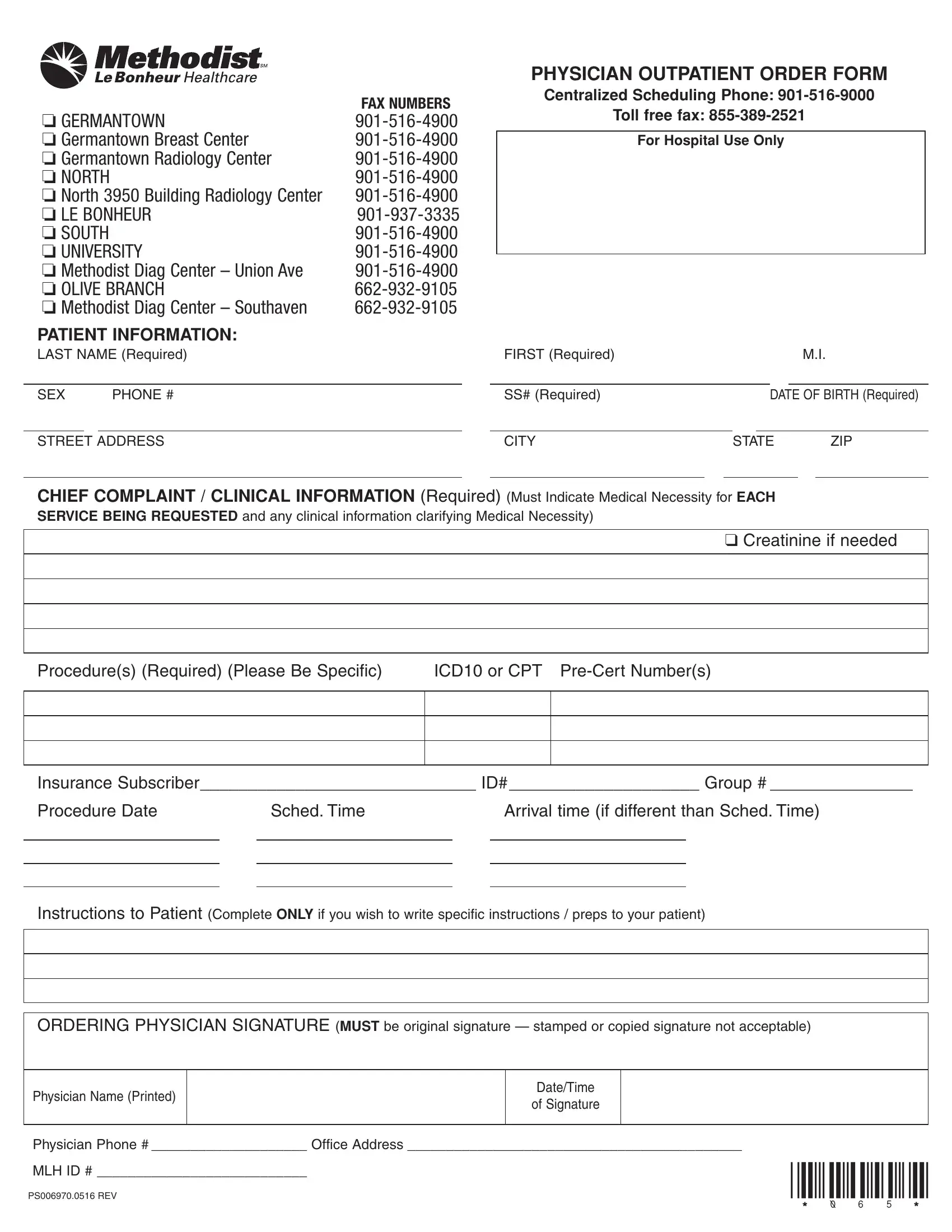
In the healthcare journey, numerous administrative steps must be navigated, one of which is the Methodist Outpatient Order form, crucial for patients requiring outpatient services within the Methodist healthcare system. This detailed document serves as a direct line of communication between the ordering physician and various departments, ensuring that all the necessary patient information and specific medical orders are accurately conveyed and understood. It includes segments for detailed patient information such as name, sex, social security number, date of birth, and contact details — all required for proper identification and processing. Additionally, it caters to the necessity for pinpointing the chief complaint or clinical reasoning behind the required services, with spaces designated for the inclusion of the requested procedures, relevant ICD10 or CPT codes, and the pre-certification numbers if applicable. A significant feature is the emphasis on the requirement for each service's medical necessity to be indicated, underlining the form's role in supporting evidence-based, necessary care. The selection of fax numbers for various Methodist locations illustrates the form's versatility in facilitating orders across multiple departments such as Radiology Centers and specialized units like the Germantown Breast Center. Moreover, the form addresses logistical details like the procedure date, scheduled time, and specific patient instructions, rounding out all necessary preparatory information. The requisite for an original signature from the ordering physician underscores the form’s legal and procedural importance, ensuring the authenticity and accountability of the outpatient order.
| Question | Answer |
|---|---|
| Form Name | Methodist Outpatient Order Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | outptform methodist north outpatient order form 2009 |
|
|
|
|
FAX NUMBERS |
❏ GERMANTOWN |
||||
❏ Germantown Breast Center |
||||
❏ Germantown Radiology Center |
||||
❏ NORTH |
|
|||
❏ North 3950 Building Radiology Center |
||||
❏ LE BONHEUR |
||||
❏ SOUTH |
|
|||
❏ UNIVERSITY |
||||
❏ Methodist Diag Center – Union Ave |
||||
❏ OLIVE BRANCH |
||||
❏ Methodist Diag Center – Southaven |
||||
PATIENT INFORMATION: |
|
|||
LAST NAME (Required) |
|
|||
|
|
|
|
|
SEX |
PHONE # |
|
||
|
|
|
|
|
PHYSICIAN OUTPATIENT ORDER FORM
Centralized Scheduling Phone:
Toll free fax:
For Hospital Use Only
FIRST (Required) |
|
|
|
M.I. |
|
|
|
|
|
SS# (Required) |
|
DATE OF BIRTH (Required) |
||
|
|
|
|
|
CITY |
STATE |
ZIP |
||
(Must Indicate Medical Necessity for EACH
SERVICE BEING REQUESTED and any clinical information clarifying Medical Necessity)
❑ Creatinine if needed
Procedure(s) (Required) (Please Be Specific) |
ICD10 or CPT |
|
|
|
|
|
|
|
|
|
|
|
|
|
Insurance Subscriber_____________________________ ID# ____________________ Group # _______________
Procedure Date |
|
Sched. Time |
|
Arrival time (if different than Sched. Time) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Instructions to Patient (Complete ONLY if you wish to write specific instructions / preps to your patient)
ORDERING PHYSICIAN SIGNATURE (MUST be original signature — stamped or copied signature not acceptable)
Physician Name (Printed)
Date/Time
of Signature
Physician Phone # ____________________ Office Address ___________________________________________
MLH ID # ___________________________ |
*065* |
|
|
PS006970.0516 REV |
|