We used the best computer programmers to create the PDF editor. Our app will allow you to prepare the metroplus health plan provider forms document with no trouble and won't consume a lot of your energy. This easy guide will enable you to start out.
Step 1: Click the "Get Form Now" button to begin.
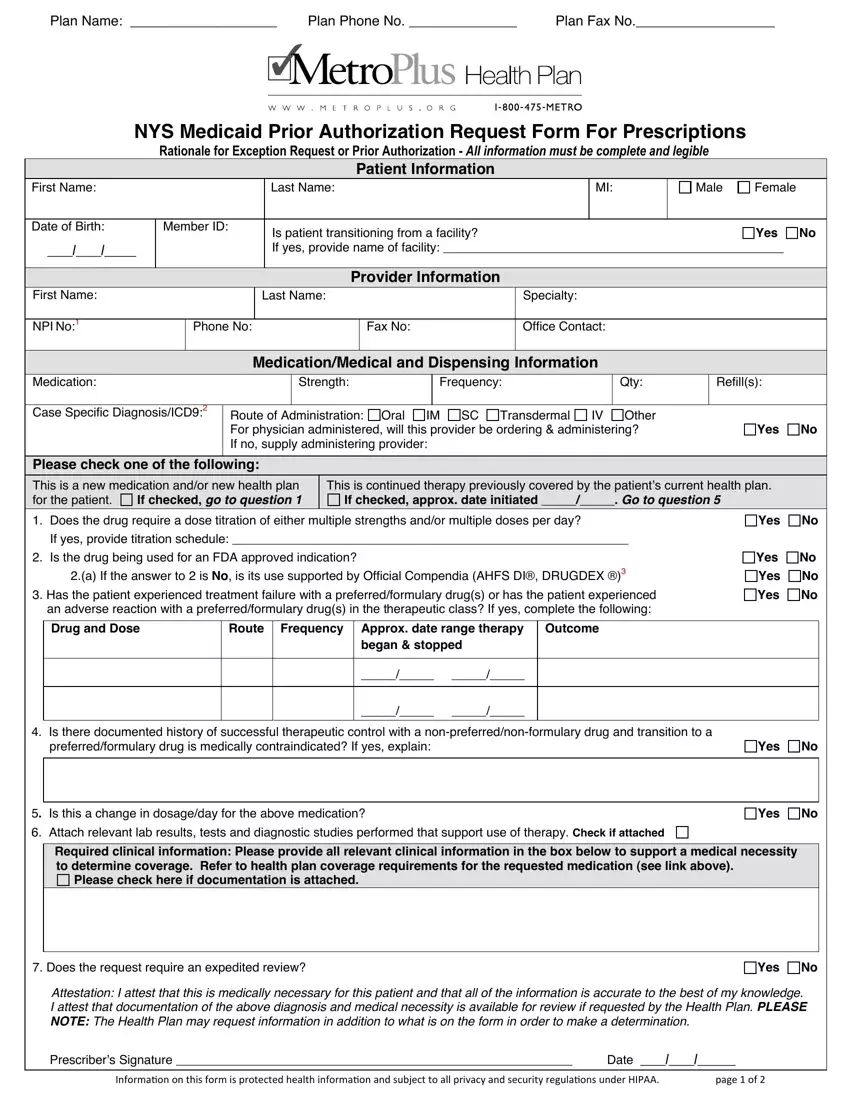
Step 2: So, you may modify the metroplus health plan provider forms. This multifunctional toolbar will let you add, delete, customize, highlight, as well as undertake other commands to the content and fields within the form.
For every single part, complete the content requested by the program.
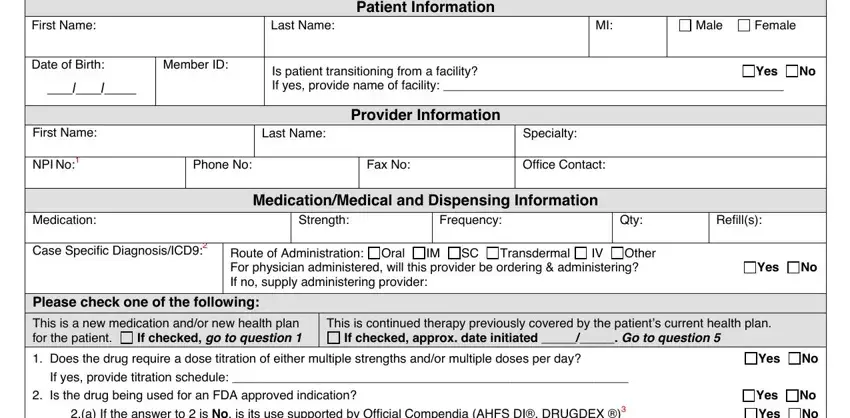
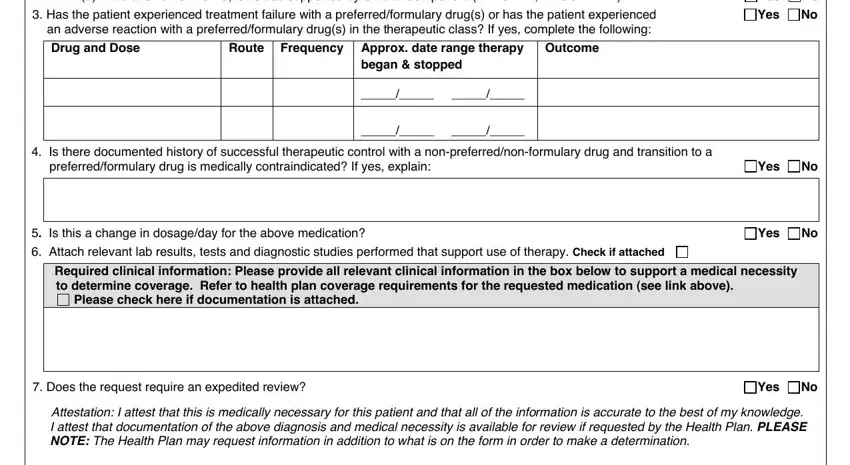
You have to enter the appropriate details in the Does the drug require a dose, No No No, an adverse reaction with a, Drug and Dose, Route Frequency Approx date range, Outcome, began stopped, Is there documented history of, preferredformulary drug is, Is this a change in dosageday for, Required clinical information, Please check here if documentation, Does the request require an, and Attestation I attest that this is field.
Step 3: Press the "Done" button. Now it's easy to export the PDF file to your electronic device. Aside from that, it is possible to forward it through electronic mail.
Step 4: It is safer to keep duplicates of the form. You can rest assured that we won't disclose or see your data.
