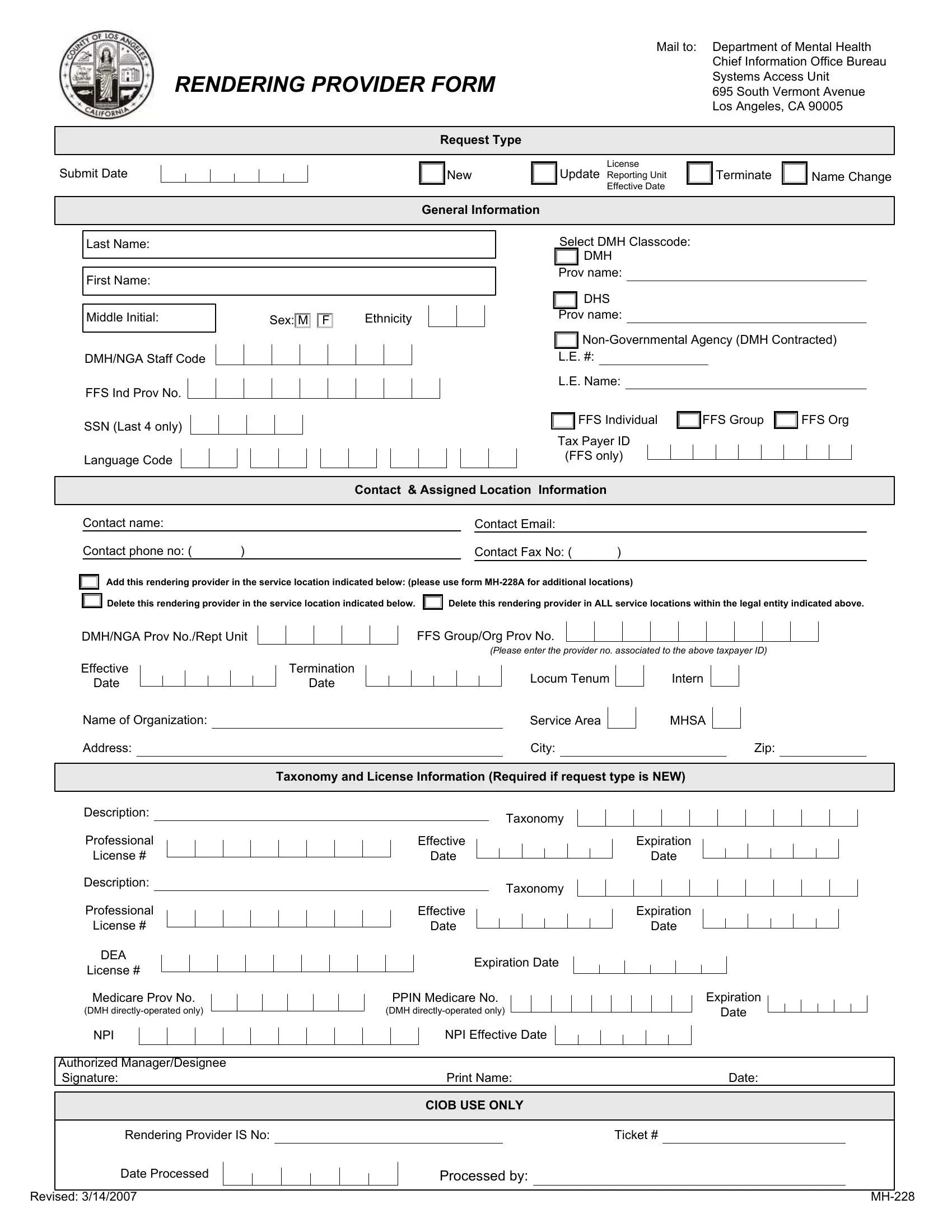
At the intersection of mental health services and administrative protocol lies the MH-228 form, a critical document for mental health professionals working within or in affiliation with the Department of Mental Health. This comprehensive form is not merely paperwork; it is a gateway for mental health providers to register, update, or terminate their professional details in an official capacity. It caters to various requests like initiating service as a new provider, updating existing information, or even going through the process of termination. Specifically, it requires detailed personal information, including names, contact details, and licensure specifics, ensuring that the mental health provider’s credentials are up to date and accurately reflected in the Department of Mental Health's records. The form also segments into identifying whether the provider is an individual, a group, or an organization, further clarifying the nature of services offered. Taxpayer IDs and other financial identifiers are crucial for those operating on a fee-for-service basis, emphasizing the form’s role in sorting out both legal and bureaucratic necessities. Aimed at facilitating better service delivery and operational efficiency, the MH-228 form stands as a testament to the organized, systematic approach adopted by the Department of Mental Health. Its careful design enables a seamless interface between mental health professionals and administrative benchmarks, ensuring that providers can focus more on delivering quality care, unencumbered by procedural complexities.
| Question | Answer |
|---|---|
| Form Name | Mh 228 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | RPfill ableNPI dmh rendering provider form |