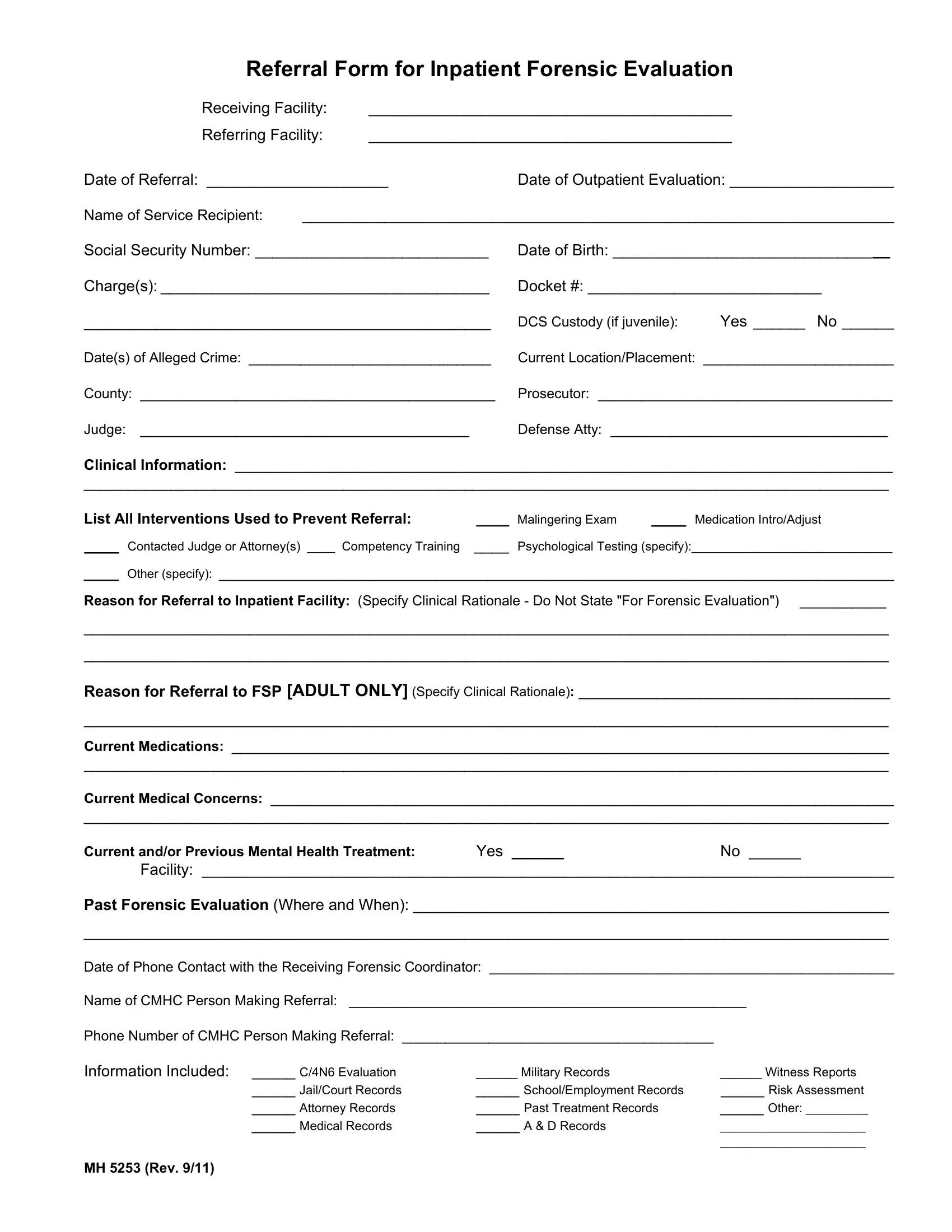
The MH 5253 form serves as a critical document in the nexus between the healthcare and legal systems, specifically tailored for referrals to inpatient forensic evaluations. Designed meticulously to account for all necessary information, this form encapsulates the essence of transferring a service recipient, who may be involved in legal proceedings, from one facility to another with a focus on their mental health needs. The structured sections demand comprehensive details such as the identification of both the receiving and referring facilities, the date of referral alongside the timing of any outpatient evaluations conducted, the service recipient's personal information including their social security number and date of birth, and the legal context marked by charges and custody status if applicable. Further, it delves into the clinical domain, seeking insights into the recipient's current mental health status, previous interventions undertaken to avert the need for an inpatient referral, the clinical rationale behind the referral, ongoing medications, medical concerns, and any historical mental health treatments. Moreover, it emphasizes the importance of including relevant documents alongside the referral, such as evaluations, military records, or risk assessments, to ensure a holistic understanding of the individual's situation. This form plays a pivotal role in bridging the informational gap between healthcare providers and the legal system, aiming to align on the best course of action for individuals at the intersection of mental health challenges and legal scrutiny.
| Question | Answer |
|---|---|
| Form Name | Form Mh 5253 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | form, 4N6, Competency, Inpatient |
