
EDD can be completed without any problem. Just open FormsPal PDF editor to get the job done right away. The tool is constantly maintained by our team, getting new functions and turning out to be better. If you are seeking to get started, here is what it's going to take:
Step 1: First, open the tool by clicking the "Get Form Button" in the top section of this page.
Step 2: The tool helps you modify your PDF form in many different ways. Change it by including your own text, adjust what's already in the document, and place in a signature - all when it's needed!
This PDF will need particular details to be filled in, so ensure that you take some time to enter what is expected:
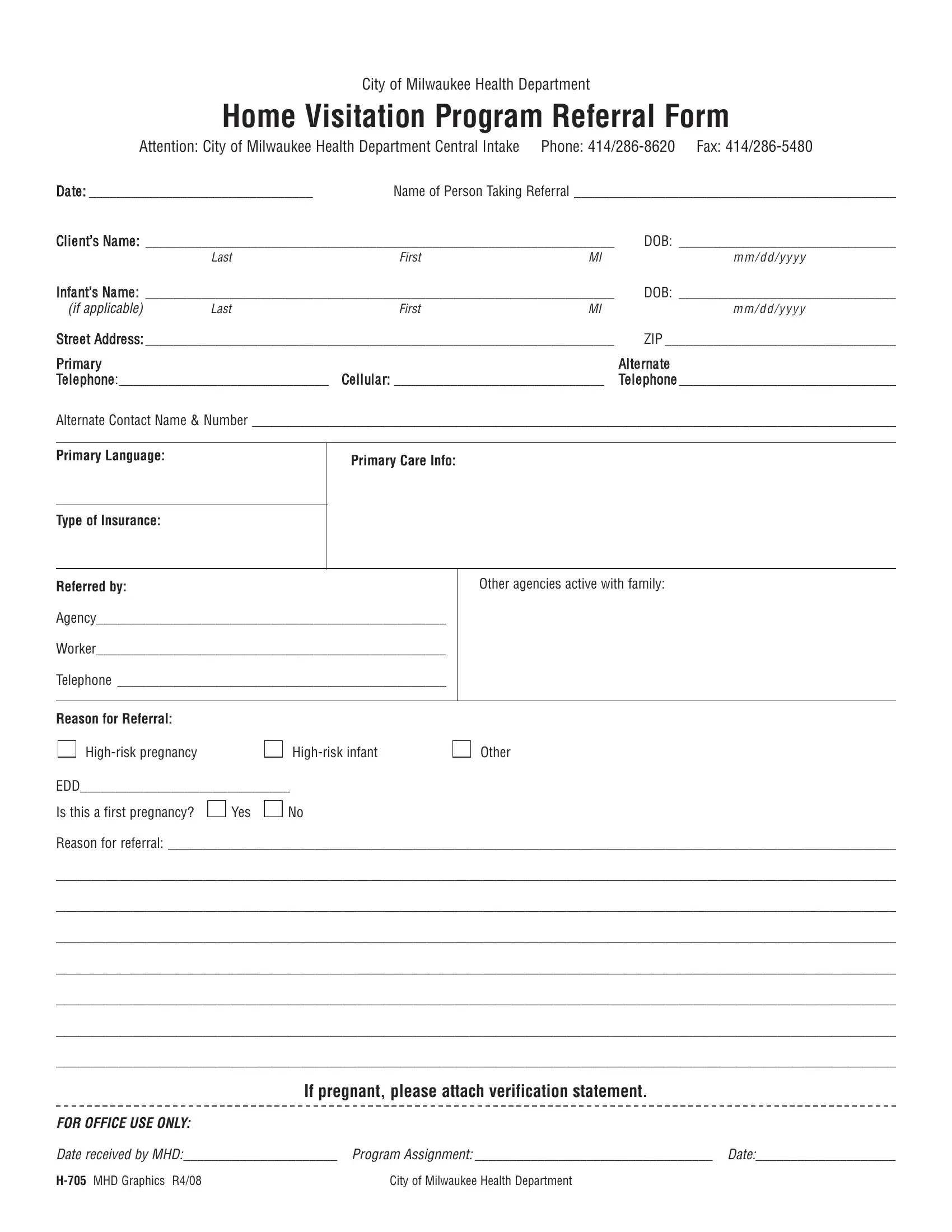
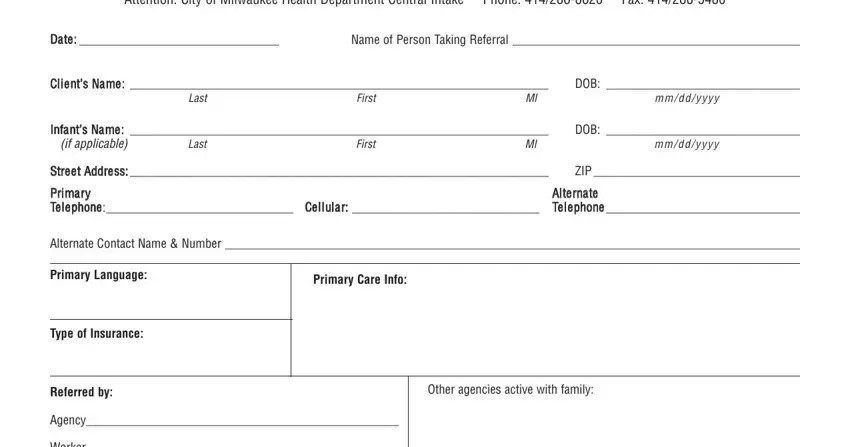
1. First of all, once filling out the EDD, beging with the part that features the subsequent blanks:
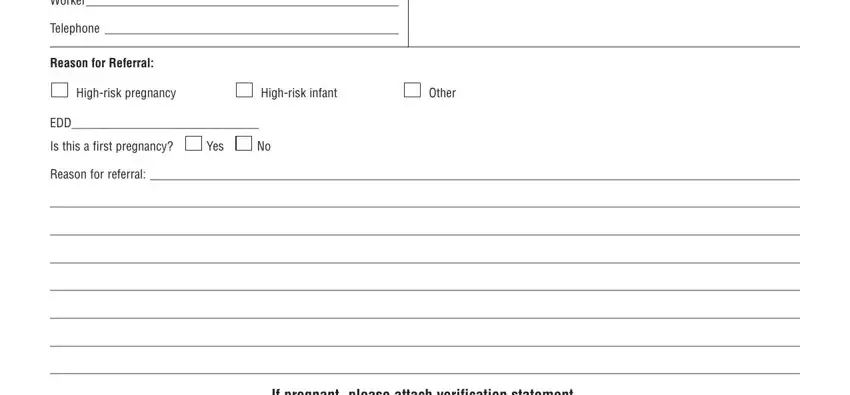
2. Just after this selection of fields is done, go to enter the suitable details in all these - Worker, Telephone, Reason for Referral, Highrisk pregnancy, Highrisk infant, Other, EDD, Is this a first pregnancy, Yes, Reason for referral, and If pregnant please attach.
3. Completing FOR OFFICE USE ONLY, Date received by MHD Program, and H MHD Graphics R City of Milwaukee is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!

Always be extremely attentive when filling out H MHD Graphics R City of Milwaukee and Date received by MHD Program, since this is where many people make a few mistakes.
Step 3: Before finalizing the file, ensure that blank fields were filled in as intended. When you believe it is all fine, click “Done." After starting afree trial account at FormsPal, it will be possible to download EDD or email it without delay. The file will also be accessible via your personal account page with all your modifications. We do not share any information that you use while filling out documents at FormsPal.